Nicolas Weiss, Clémence Marois, Loic Le Guennec, Benjamin Rohaut, Sophie Demeret
{"title":"Critical insights for intensivists on Guillain-Barré syndrome.","authors":"Nicolas Weiss, Clémence Marois, Loic Le Guennec, Benjamin Rohaut, Sophie Demeret","doi":"10.1186/s13613-025-01464-w","DOIUrl":null,"url":null,"abstract":"<p><p>Guillain-Barré Syndrome (GBS) is a leading cause of acute flaccid tetraplegia worldwide, with an incidence of 1-2 cases per 100,000 people per year. Characterized by an immune-mediated polyneuropathy, GBS often follows infections or immunological triggers, including vaccinations. The syndrome is classified into three main subtypes based on electrophysiological findings: acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), and acute motor sensory axonal neuropathy (AMSAN). The pathophysiology of GBS involves molecular mimicry between microbial antigens and nerve structures, particularly affecting gangliosides and myelin proteins. Diagnosis primarily relies on clinical history, with lumbar puncture and electroneuromyogram used to confirm and differentiate subtypes. Treatment includes intravenous immunoglobulins or therapeutic plasma exchange associated with symptomatic treatment, especially mechanical ventilation if needed. Prognosis is generally favorable with a low mortality rate (< 5%) overall, but neurological sequelae can occur. Current research continues to explore novel therapeutic approaches, including complement-targeted therapies. Despite advancements, progress in specific treatments has been limited, and ongoing evaluation of potential biomarkers such as neurofilament light chains may enhance prognosis prediction and management strategies.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"67"},"PeriodicalIF":5.5000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12092332/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01464-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
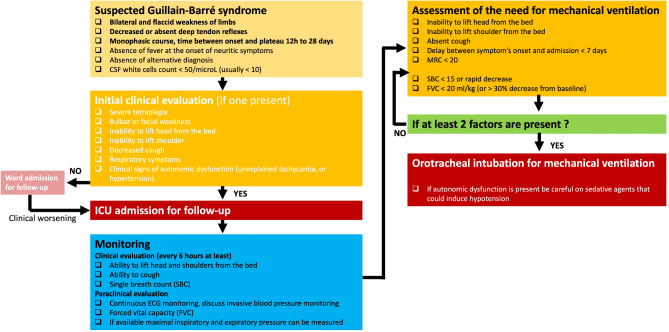
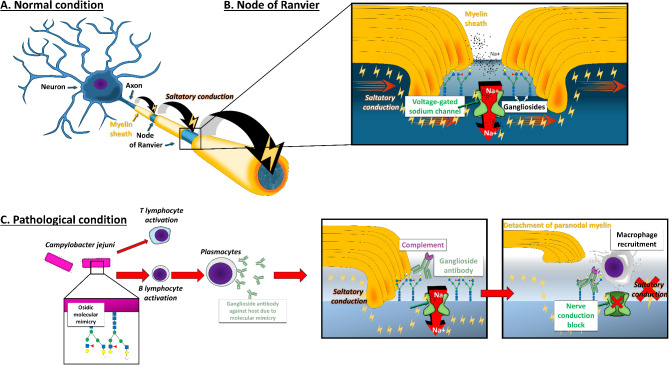
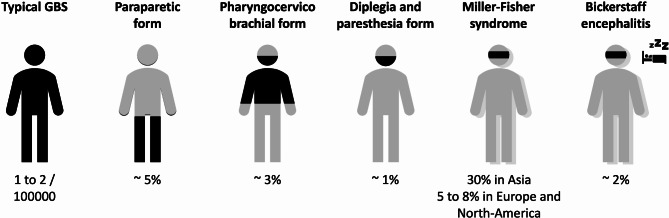
Guillain-Barré Syndrome (GBS) is a leading cause of acute flaccid tetraplegia worldwide, with an incidence of 1-2 cases per 100,000 people per year. Characterized by an immune-mediated polyneuropathy, GBS often follows infections or immunological triggers, including vaccinations. The syndrome is classified into three main subtypes based on electrophysiological findings: acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), and acute motor sensory axonal neuropathy (AMSAN). The pathophysiology of GBS involves molecular mimicry between microbial antigens and nerve structures, particularly affecting gangliosides and myelin proteins. Diagnosis primarily relies on clinical history, with lumbar puncture and electroneuromyogram used to confirm and differentiate subtypes. Treatment includes intravenous immunoglobulins or therapeutic plasma exchange associated with symptomatic treatment, especially mechanical ventilation if needed. Prognosis is generally favorable with a low mortality rate (< 5%) overall, but neurological sequelae can occur. Current research continues to explore novel therapeutic approaches, including complement-targeted therapies. Despite advancements, progress in specific treatments has been limited, and ongoing evaluation of potential biomarkers such as neurofilament light chains may enhance prognosis prediction and management strategies.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


