Association between ventilation-perfusion matching improvement during initial prone positioning and ICU mortality in patients with moderate to severe ARDS: a prospective two-center study.
{"title":"Association between ventilation-perfusion matching improvement during initial prone positioning and ICU mortality in patients with moderate to severe ARDS: a prospective two-center study.","authors":"Rui Wang, Wancong Wang, Xiao Tang, Zhenyuan Qi, Ting Li, Yalan Liu, Hongju Li, Jican Yan, Hua Yang, Wenrui Lyu, Zhaohong Li, Bing Sun, Guifen Gan","doi":"10.1186/s13613-025-01489-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prone positioning (PP) is widely used in patients with moderate to severe acute respiratory distress syndrome (ARDS) to reduce mortality by mitigating the risk of ventilation-induced lung injury (VILI) and enhancing ventilation-perfusion (V/Q) matching. However, patient responses to PP are variable, and the relationship between V/Q matching improvement during PP and clinical outcomes remains unclear. This study aimed to test the hypothesis that improvements in V/Q matching 4 h within the first PP are associated with reduced intensive care unit (ICU) mortality.</p><p><strong>Methods: </strong>In this two-center, prospective, observational study, regional ventilation and perfusion changes in patients with moderate to severe ARDS were evaluated using electrical impedance tomography (EIT) during the first PP session. Patients were categorized as responders or non-responders based on whether V/Q matching improved by ≥ 10% within 4 h of the first PP. The primary endpoint was ICU mortality, and the secondary endpoint was ventilator-free days at day 28.</p><p><strong>Results: </strong>A total of 77 patients were included in the study, with 46 (59.7%) classified as responders and 31 (40.3%) as non-responders. EIT revealed significant improvements in V/Q matching during PP, primarily through reduced dorsal shunt and ventral dead space. These improvements were partially sustained after resupination. Responders showed significantly lower ICU mortality (28.3% vs. 51.6%; P = 0.038) and more ventilator-free days at day 28 (16 [range, 0-21] days vs. 9 [0-15] days; P = 0.024) than non-responders. Multivariate analysis confirmed enhanced V/Q matching as an independent protective factor against mortality (OR, 0.790; 95% CI, 0.681-0.917; P = 0.002).</p><p><strong>Conclusions: </strong>Improvement in V/Q matching 4 h within the first PP is associated with lower ICU mortality in patients with moderate to severe ARDS. These findings underscore the importance of PP in ARDS management and highlight the potential of V/Q responsiveness in guiding individualized PP strategies.</p><p><strong>Trial registration: </strong>ClinicalTrials.Gov: NCT05765760. Registered 28 February 2023.</p>","PeriodicalId":7966,"journal":{"name":"Annals of Intensive Care","volume":"15 1","pages":"69"},"PeriodicalIF":5.5000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12092903/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13613-025-01489-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prone positioning (PP) is widely used in patients with moderate to severe acute respiratory distress syndrome (ARDS) to reduce mortality by mitigating the risk of ventilation-induced lung injury (VILI) and enhancing ventilation-perfusion (V/Q) matching. However, patient responses to PP are variable, and the relationship between V/Q matching improvement during PP and clinical outcomes remains unclear. This study aimed to test the hypothesis that improvements in V/Q matching 4 h within the first PP are associated with reduced intensive care unit (ICU) mortality.
Methods: In this two-center, prospective, observational study, regional ventilation and perfusion changes in patients with moderate to severe ARDS were evaluated using electrical impedance tomography (EIT) during the first PP session. Patients were categorized as responders or non-responders based on whether V/Q matching improved by ≥ 10% within 4 h of the first PP. The primary endpoint was ICU mortality, and the secondary endpoint was ventilator-free days at day 28.
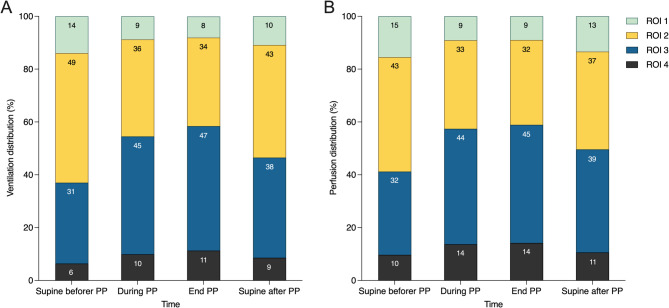
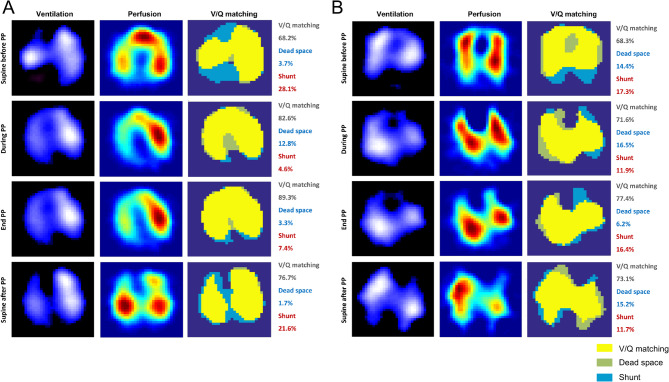
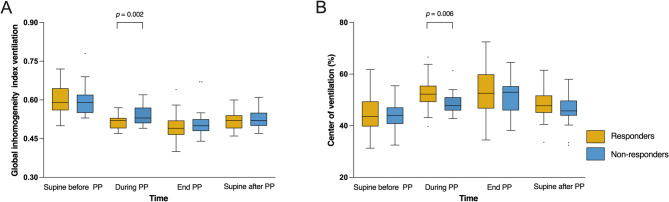
Results: A total of 77 patients were included in the study, with 46 (59.7%) classified as responders and 31 (40.3%) as non-responders. EIT revealed significant improvements in V/Q matching during PP, primarily through reduced dorsal shunt and ventral dead space. These improvements were partially sustained after resupination. Responders showed significantly lower ICU mortality (28.3% vs. 51.6%; P = 0.038) and more ventilator-free days at day 28 (16 [range, 0-21] days vs. 9 [0-15] days; P = 0.024) than non-responders. Multivariate analysis confirmed enhanced V/Q matching as an independent protective factor against mortality (OR, 0.790; 95% CI, 0.681-0.917; P = 0.002).
Conclusions: Improvement in V/Q matching 4 h within the first PP is associated with lower ICU mortality in patients with moderate to severe ARDS. These findings underscore the importance of PP in ARDS management and highlight the potential of V/Q responsiveness in guiding individualized PP strategies.
Trial registration: ClinicalTrials.Gov: NCT05765760. Registered 28 February 2023.
期刊介绍:
Annals of Intensive Care is an online peer-reviewed journal that publishes high-quality review articles and original research papers in the field of intensive care medicine. It targets critical care providers including attending physicians, fellows, residents, nurses, and physiotherapists, who aim to enhance their knowledge and provide optimal care for their patients. The journal's articles are included in various prestigious databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, OCLC, PubMed, PubMed Central, Science Citation Index Expanded, SCOPUS, and Summon by Serial Solutions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


