Ladan Salamati, Bahar Dehghan, Mohammad Reza Sabri, Alireza Ahmadi, Mehdi Ghaderian, Chehreh Mahdavi, Davood Ramezani Nezhad, Atefeh Karbasi, Mohsen Sedighi
{"title":"Caffeine Treatment for Prostaglandin E1-Induced Apnea Prevention in Congenital Heart Disease Neonates: A Randomized Clinical Trial.","authors":"Ladan Salamati, Bahar Dehghan, Mohammad Reza Sabri, Alireza Ahmadi, Mehdi Ghaderian, Chehreh Mahdavi, Davood Ramezani Nezhad, Atefeh Karbasi, Mohsen Sedighi","doi":"10.1155/ccrp/4923280","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Congenital heart diseases (CHDs) are structural abnormalities of the heart or great vessels. Prostaglandin E1 (PGE1) is used to maintain the ductus arteriosus open in neonates with ductal-dependent heart lesions but is associated with apnea. We aimed to investigate the effects of caffeine therapy on the occurrence of apnea in neonates with CHD. <b>Methods:</b> This single-blinded randomized clinical trial was performed on 51 CHD neonates who were treated with PGE1 or PGE1 + caffeine. PGE1 dose ranged from 0.01 to 0.1 mcg/kg/min, and caffeine was administered initially at 20 mg/kg, followed by a daily bolus dose of 10 mg/kg. Demographic and clinical data, prevalence of apnea, and PGE1 side effects were recorded and analyzed. <b>Results:</b> A total of 51 CHD neonates receiving PGE1 + caffeine (<i>n</i> = 25) and PGE1 (<i>n</i> = 26) were included. The median age of total neonates was 2 (1-7) days, and 57% were female. There was no statistically significant difference between the baseline characteristics of participants, but neonates in the caffeine group received a higher mean dose of PGE1 (0.03 ± 0.17 vs. 0.02 ± 0.02, <i>p</i>=0.049) over the course of the treatment. The prevalence of apnea was 20% in the PGE1 + caffeine group and 42% in the PGE1 group (<i>p</i>=0.086). In the Cox regression model, the age of neonates had a significant effect on time to apnea in patients receiving caffeine (HR = 0.87, <i>p</i>=0.04). <b>Conclusion:</b> Our findings fail to demonstrate that caffeine therapy reduces PGE1-induced apnea. A larger randomized controlled trial is required to confirm or refute the efficacy of caffeine in reducing the incidence of apnea associated with PGE1 infusion. <b>Trial Registration:</b> Iranian Registry of Clinical Trials: IRCT20220503054729N1.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2025 ","pages":"4923280"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12086028/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/ccrp/4923280","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
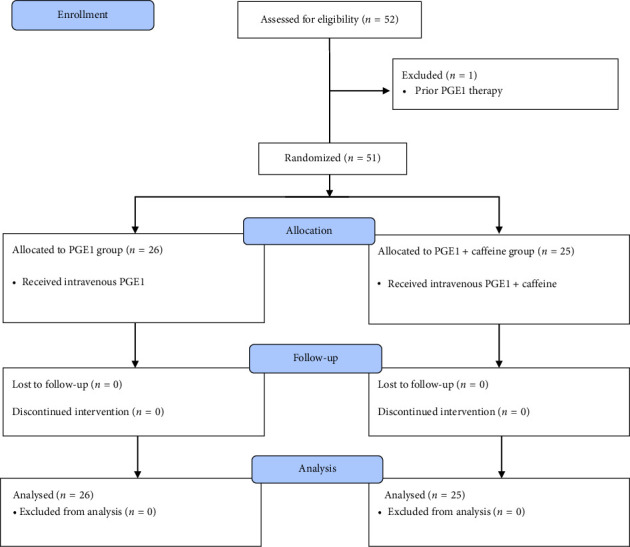
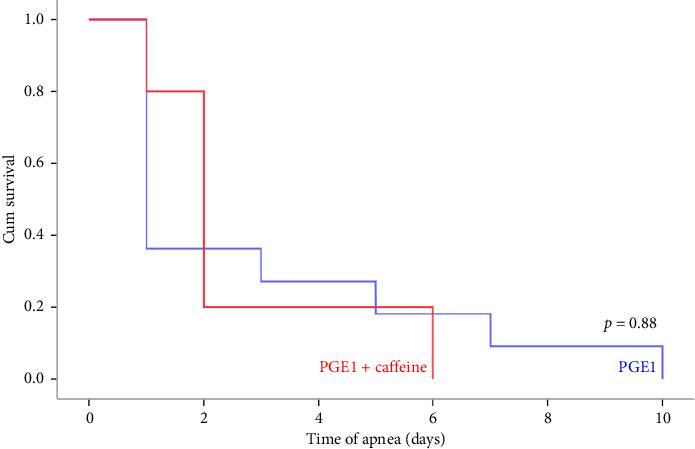
Background: Congenital heart diseases (CHDs) are structural abnormalities of the heart or great vessels. Prostaglandin E1 (PGE1) is used to maintain the ductus arteriosus open in neonates with ductal-dependent heart lesions but is associated with apnea. We aimed to investigate the effects of caffeine therapy on the occurrence of apnea in neonates with CHD. Methods: This single-blinded randomized clinical trial was performed on 51 CHD neonates who were treated with PGE1 or PGE1 + caffeine. PGE1 dose ranged from 0.01 to 0.1 mcg/kg/min, and caffeine was administered initially at 20 mg/kg, followed by a daily bolus dose of 10 mg/kg. Demographic and clinical data, prevalence of apnea, and PGE1 side effects were recorded and analyzed. Results: A total of 51 CHD neonates receiving PGE1 + caffeine (n = 25) and PGE1 (n = 26) were included. The median age of total neonates was 2 (1-7) days, and 57% were female. There was no statistically significant difference between the baseline characteristics of participants, but neonates in the caffeine group received a higher mean dose of PGE1 (0.03 ± 0.17 vs. 0.02 ± 0.02, p=0.049) over the course of the treatment. The prevalence of apnea was 20% in the PGE1 + caffeine group and 42% in the PGE1 group (p=0.086). In the Cox regression model, the age of neonates had a significant effect on time to apnea in patients receiving caffeine (HR = 0.87, p=0.04). Conclusion: Our findings fail to demonstrate that caffeine therapy reduces PGE1-induced apnea. A larger randomized controlled trial is required to confirm or refute the efficacy of caffeine in reducing the incidence of apnea associated with PGE1 infusion. Trial Registration: Iranian Registry of Clinical Trials: IRCT20220503054729N1.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


