Melissa R Requist, Andrew C Peterson, Timothy C Beals, Bopha Chrea, Amy L Lenz
{"title":"Osseous morphology differences in the foot and ankle associated with Charcot-Marie-Tooth disease.","authors":"Melissa R Requist, Andrew C Peterson, Timothy C Beals, Bopha Chrea, Amy L Lenz","doi":"10.1093/jbmrpl/ziaf058","DOIUrl":null,"url":null,"abstract":"<p><p>Charcot-Marie-Tooth (CMT) disease is a genetic, progressive peripheral nerve disease that commonly manifests in a cavovarus foot deformity. Previously, this foot deformity has been believed to be an alignment change in the foot, but recent research has shown that there are bone morphology differences in individuals with CMT. Differences in bone morphology have been identified in the calcaneus, talus, and medial cuneiform, but have not been consistently analyzed throughout the foot or studied in relation to different genetic subtypes of CMT. This study is a retrospective, cross-sectional analysis of bone morphology in CMT using weight-bearing computed tomography and statistical shape modeling. This analysis identified bone morphology differences between CMT and control groups throughout the hindfoot, midfoot, and forefoot. Bone morphology differences were also present between the 2 primary disease subtypes throughout the foot. Key morphologic findings include the altered shape of the subtalar articular surfaces on the talus, bending of the metatarsals, variation in navicular process morphology, and differences between subtypes in the talus, medial cuneiform, and medial metatarsals. There are several possible theoretical mechanisms for this osseous deformation, including bone remodeling in response to altered loading from alignment change or from decreased musculotendinous forces, but the patterns of morphological variation seen in these data cannot be fully explained by these mechanisms, suggesting that there may be an interaction between the neuronal disease and bone remodeling. Future work is necessary to characterize the progression of bony deformity throughout development and to correlate bone shape with function, gait, muscle morphology and strength to elucidate the mechanism of osseous morphology change in varying subtypes of CMT.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"9 6","pages":"ziaf058"},"PeriodicalIF":2.4000,"publicationDate":"2025-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12087961/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziaf058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
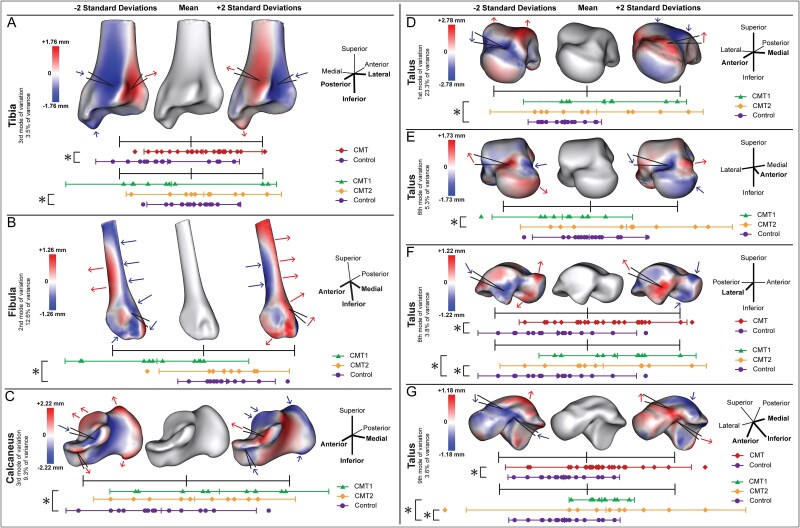
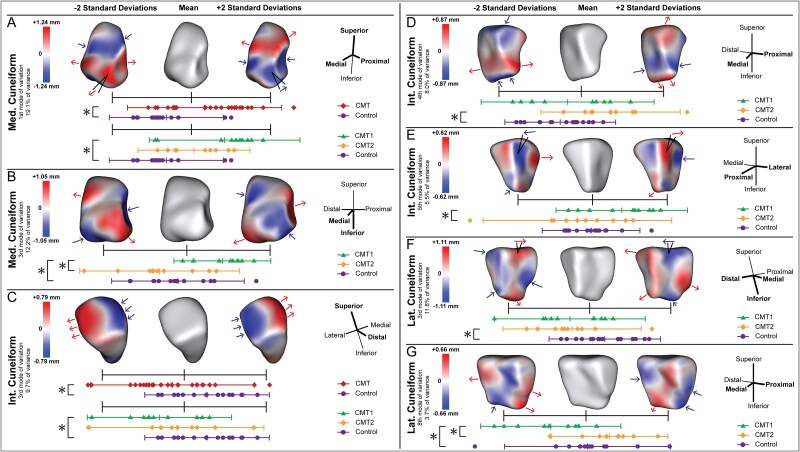
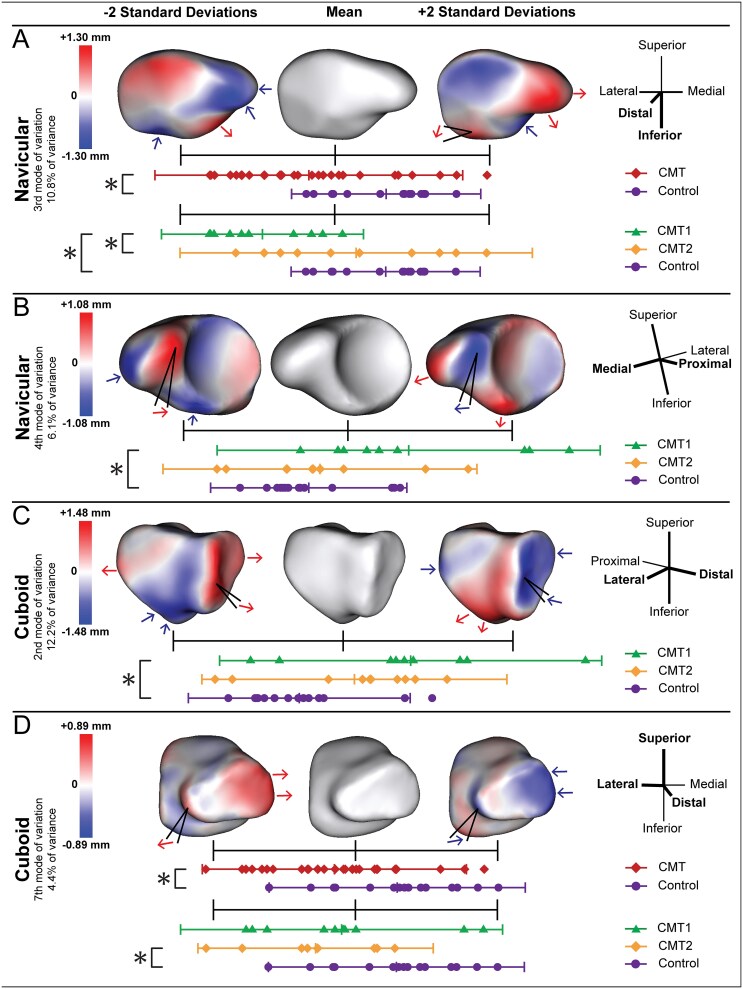
Charcot-Marie-Tooth (CMT) disease is a genetic, progressive peripheral nerve disease that commonly manifests in a cavovarus foot deformity. Previously, this foot deformity has been believed to be an alignment change in the foot, but recent research has shown that there are bone morphology differences in individuals with CMT. Differences in bone morphology have been identified in the calcaneus, talus, and medial cuneiform, but have not been consistently analyzed throughout the foot or studied in relation to different genetic subtypes of CMT. This study is a retrospective, cross-sectional analysis of bone morphology in CMT using weight-bearing computed tomography and statistical shape modeling. This analysis identified bone morphology differences between CMT and control groups throughout the hindfoot, midfoot, and forefoot. Bone morphology differences were also present between the 2 primary disease subtypes throughout the foot. Key morphologic findings include the altered shape of the subtalar articular surfaces on the talus, bending of the metatarsals, variation in navicular process morphology, and differences between subtypes in the talus, medial cuneiform, and medial metatarsals. There are several possible theoretical mechanisms for this osseous deformation, including bone remodeling in response to altered loading from alignment change or from decreased musculotendinous forces, but the patterns of morphological variation seen in these data cannot be fully explained by these mechanisms, suggesting that there may be an interaction between the neuronal disease and bone remodeling. Future work is necessary to characterize the progression of bony deformity throughout development and to correlate bone shape with function, gait, muscle morphology and strength to elucidate the mechanism of osseous morphology change in varying subtypes of CMT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


