{"title":"National and Subnational Burden of Cardiovascular Diseases in Iran from 1990 to 2021: Results from Global Burden of Diseases 2021 study.","authors":"Mahsa Heidari-Foroozan, Melina Farshbafnadi, Ali Golestani, Sepehr Younesian, Hosein Jafary, Mohammad-Mahdi Rashidi, Ozra Tabatabaei-Malazy, Nazila Rezaei, Mostafa Moghimi Kheirabady, Arash Bagherian Ghotbi, Seyyed-Hadi Ghamari","doi":"10.5334/gh.1429","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In 2021, cardiovascular diseases (CVD) caused around 20.5 million deaths worldwide, making them a major health concern.</p><p><strong>Methods: </strong>Incidence, prevalence, death, years of life lost (YLL), years lived with disability (YLD), and disability-adjusted life years (DALYs) were the burden measures that were assessed. All measures are reported as both all-age numbers and age-standardized rates (ASR) with 95% uncertainty intervals (UI). Decomposition analysis was conducted on CVD incidence.</p><p><strong>Results: </strong>From 1990 to 2021, all-age CVD prevalence in Iran increased by 182.6% (2.9 to 8.3 million cases), with males consistently showing higher age-standardized prevalence rates (ASPR) than females (11,350 vs. 9,431 per 100,000 in 2021). ASPR remained stable nationally (9,956 to 10,386 per 100,000), peaking in adults ≥80 years. Incident cases rose by 159.6% (0.36 to 0.92 million), driven by population growth (49.5%) and aging (136.2%), while age-standardized incidence rates (ASIR) declined by 28.3% (1,337 to 1,197 per 100,000); with males (1,336) exhibiting higher rates than females (1,060) in 2021. All age deaths doubled (86,527 to 169,582) during this period, but age-standardized death rates (ASDR) decreased substantially by 42.97% (446 to 255 per 100,000). DALYs increased by 53.7% (2.4 to 3.7 million), though age-standardized DALY rates dropped 45.3% (9,096 to 4,977 per 100,000), dominated by ischemic heart disease (2,731 ASR) and stroke (1,229 ASR). High systolic blood pressure, dietary risks, and LDL cholesterol remained the leading contributors to DALYs nationwide.</p><p><strong>Conclusion: </strong>Iran's rising CVD burden demands prioritizing cardiac care infrastructure in underserved provinces like Golestan, enforcing sodium reduction policies aligned with Iran's existing trans-fat regulations, and integrating sex-specific programs such as tobacco control for males and community hypertension screening for women are critical. Multisectoral collaboration, including urban design promoting physical activity and subsidies for whole grains, must address provincial inequities exacerbated by Iran's aging population and dietary risks.</p>","PeriodicalId":56018,"journal":{"name":"Global Heart","volume":"20 1","pages":"43"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12083073/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Heart","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5334/gh.1429","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In 2021, cardiovascular diseases (CVD) caused around 20.5 million deaths worldwide, making them a major health concern.
Methods: Incidence, prevalence, death, years of life lost (YLL), years lived with disability (YLD), and disability-adjusted life years (DALYs) were the burden measures that were assessed. All measures are reported as both all-age numbers and age-standardized rates (ASR) with 95% uncertainty intervals (UI). Decomposition analysis was conducted on CVD incidence.
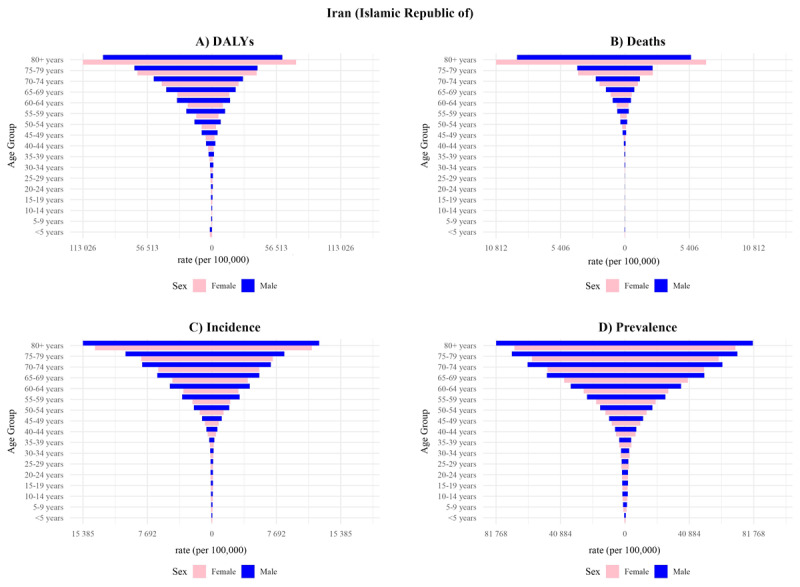
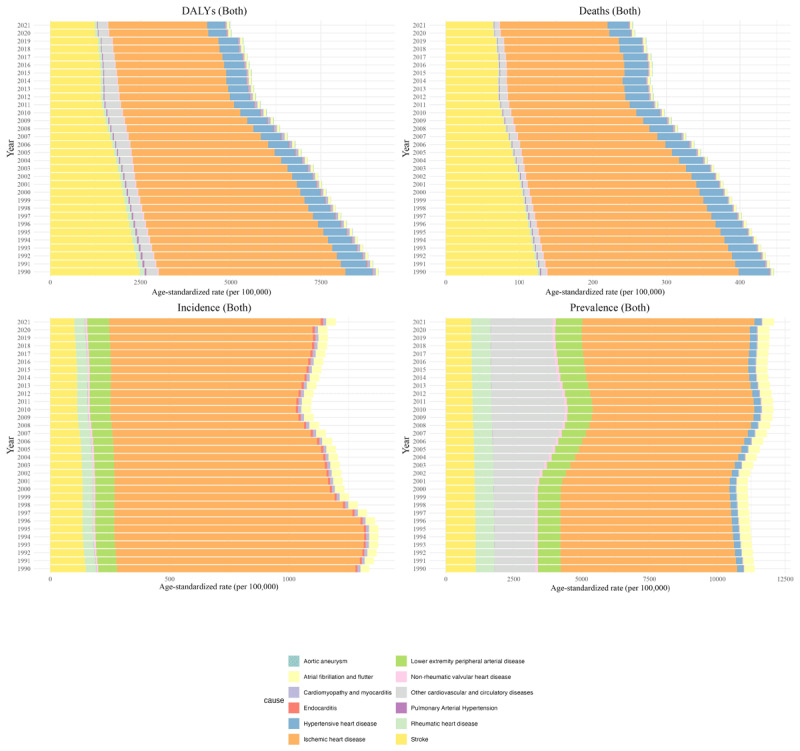
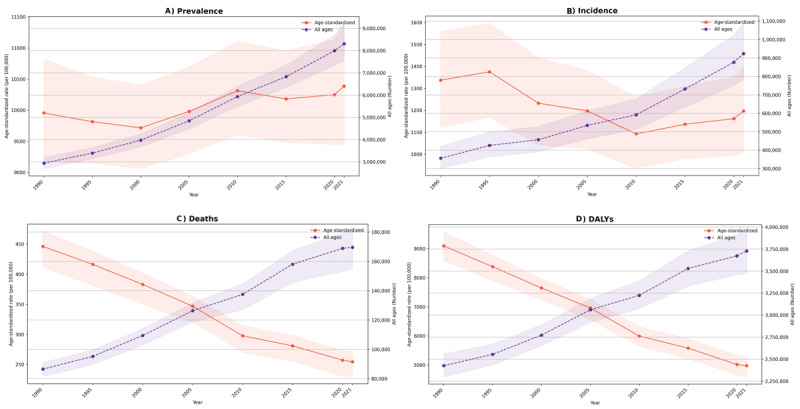
Results: From 1990 to 2021, all-age CVD prevalence in Iran increased by 182.6% (2.9 to 8.3 million cases), with males consistently showing higher age-standardized prevalence rates (ASPR) than females (11,350 vs. 9,431 per 100,000 in 2021). ASPR remained stable nationally (9,956 to 10,386 per 100,000), peaking in adults ≥80 years. Incident cases rose by 159.6% (0.36 to 0.92 million), driven by population growth (49.5%) and aging (136.2%), while age-standardized incidence rates (ASIR) declined by 28.3% (1,337 to 1,197 per 100,000); with males (1,336) exhibiting higher rates than females (1,060) in 2021. All age deaths doubled (86,527 to 169,582) during this period, but age-standardized death rates (ASDR) decreased substantially by 42.97% (446 to 255 per 100,000). DALYs increased by 53.7% (2.4 to 3.7 million), though age-standardized DALY rates dropped 45.3% (9,096 to 4,977 per 100,000), dominated by ischemic heart disease (2,731 ASR) and stroke (1,229 ASR). High systolic blood pressure, dietary risks, and LDL cholesterol remained the leading contributors to DALYs nationwide.
Conclusion: Iran's rising CVD burden demands prioritizing cardiac care infrastructure in underserved provinces like Golestan, enforcing sodium reduction policies aligned with Iran's existing trans-fat regulations, and integrating sex-specific programs such as tobacco control for males and community hypertension screening for women are critical. Multisectoral collaboration, including urban design promoting physical activity and subsidies for whole grains, must address provincial inequities exacerbated by Iran's aging population and dietary risks.
Global HeartMedicine-Cardiology and Cardiovascular Medicine
CiteScore
5.70
自引率
5.40%
发文量
77
审稿时长
5 weeks
期刊介绍:
Global Heart offers a forum for dialogue and education on research, developments, trends, solutions and public health programs related to the prevention and control of cardiovascular diseases (CVDs) worldwide, with a special focus on low- and middle-income countries (LMICs). Manuscripts should address not only the extent or epidemiology of the problem, but also describe interventions to effectively control and prevent CVDs and the underlying factors. The emphasis should be on approaches applicable in settings with limited resources.
Economic evaluations of successful interventions are particularly welcome. We will also consider negative findings if important. While reports of hospital or clinic-based treatments are not excluded, particularly if they have broad implications for cost-effective disease control or prevention, we give priority to papers addressing community-based activities. We encourage submissions on cardiovascular surveillance and health policies, professional education, ethical issues and technological innovations related to prevention.
Global Heart is particularly interested in publishing data from updated national or regional demographic health surveys, World Health Organization or Global Burden of Disease data, large clinical disease databases or registries. Systematic reviews or meta-analyses on globally relevant topics are welcome. We will also consider clinical research that has special relevance to LMICs, e.g. using validated instruments to assess health-related quality-of-life in patients from LMICs, innovative diagnostic-therapeutic applications, real-world effectiveness clinical trials, research methods (innovative methodologic papers, with emphasis on low-cost research methods or novel application of methods in low resource settings), and papers pertaining to cardiovascular health promotion and policy (quantitative evaluation of health programs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


