{"title":"Octreotide infusion pump in patients with functional neuroendocrine tumors and refractory hormonal syndrome.","authors":"Kalyan Mansukhbhai Shekhda, Eleni Armeni, Dalvinder Mandair, Aspasia Manta, George Parker, Akanksha Sarma, Aimee Hayes, Martyn Caplin, Christos Toumpanakis","doi":"10.1530/EO-25-0016","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate clinical outcomes, safety and survival measures of octreotide infusion pump (OIP) therapy in patients with metastatic neuroendocrine tumors (NETs) and refractory hormonal syndrome.</p><p><strong>Design: </strong>A retrospective analysis was conducted using data from patients treated with OIP therapy at a single center.</p><p><strong>Methods: </strong>Data on demographics, disease characteristics, biochemical profiles and treatment outcomes were extracted from electronic patient records.</p><p><strong>Results: </strong>Eighteen patients with NETs and debilitating symptoms refractory to maximum approved doses of somatostatin analogs (SSTAs) were included. The cohort comprised 18 patients (12 males (67%) and six females (33%)) with a median age of 64.5 years (IQR: 49.5-71). The most common tumor site was midgut (72.2%), followed by pancreas (22.2%). Refractory carcinoid syndrome was the primary indication for initiation of OIP therapy in 15 patients and VIPoma in three. Most tumors were WHO grade 1 or 2 (89%), and liver metastases were prevalent (94% of patients). At presentation, the median 24-h urinary 5-hydroxyindoleacetic acid (5-HIAA) level was 421.5 μmoL/24 h (<i>n</i>: 8). The mean starting OIP dose was 1,632 ± 522 μg/24 h, escalating to 2,166.7 ± 464 μg/24 h in 66.57% of patients. Symptomatic improvement was observed in 72% of patients, significantly reducing flushing and diarrhea. Patients who did not respond well to OIP therapy had more disease burden and had received more treatment lines before being started on OIP therapy.</p><p><strong>Conclusion: </strong>OIP therapy is an effective treatment option for symptom control in patients with refractory NET-related hormonal syndrome. Randomized controlled trials are warranted to confirm these findings and assess long-term outcomes.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"5 1","pages":"e250016"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12084797/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-25-0016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate clinical outcomes, safety and survival measures of octreotide infusion pump (OIP) therapy in patients with metastatic neuroendocrine tumors (NETs) and refractory hormonal syndrome.
Design: A retrospective analysis was conducted using data from patients treated with OIP therapy at a single center.
Methods: Data on demographics, disease characteristics, biochemical profiles and treatment outcomes were extracted from electronic patient records.
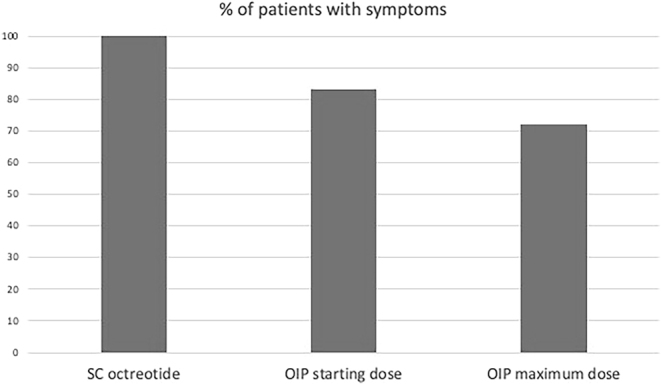
Results: Eighteen patients with NETs and debilitating symptoms refractory to maximum approved doses of somatostatin analogs (SSTAs) were included. The cohort comprised 18 patients (12 males (67%) and six females (33%)) with a median age of 64.5 years (IQR: 49.5-71). The most common tumor site was midgut (72.2%), followed by pancreas (22.2%). Refractory carcinoid syndrome was the primary indication for initiation of OIP therapy in 15 patients and VIPoma in three. Most tumors were WHO grade 1 or 2 (89%), and liver metastases were prevalent (94% of patients). At presentation, the median 24-h urinary 5-hydroxyindoleacetic acid (5-HIAA) level was 421.5 μmoL/24 h (n: 8). The mean starting OIP dose was 1,632 ± 522 μg/24 h, escalating to 2,166.7 ± 464 μg/24 h in 66.57% of patients. Symptomatic improvement was observed in 72% of patients, significantly reducing flushing and diarrhea. Patients who did not respond well to OIP therapy had more disease burden and had received more treatment lines before being started on OIP therapy.
Conclusion: OIP therapy is an effective treatment option for symptom control in patients with refractory NET-related hormonal syndrome. Randomized controlled trials are warranted to confirm these findings and assess long-term outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


