{"title":"Conducting a registry-based randomised trial (REDOX) in chronic respiratory failure: experiences and advice.","authors":"Josefin Sundh, Magnus Ekström","doi":"10.1080/20018525.2025.2502237","DOIUrl":null,"url":null,"abstract":"<p><p>Registry-based randomised controlled trials (R-RCTs) represent a paradigm shift in research, with the potential to accomplish pragmatic but large trials with high external validity. In this paper, we review our experiences from planning and performing the <i>REgistry-based randomised controlled trial of treatment Duration and mortality in long-term OXygen therapy (REDOX) trial</i>, the first R-RCT within respiratory medicine. The REDOX study compared the two established treatment options of home oxygen 15 and 24 h per day. Previous recommendations to use oxygen for at least 15 h but preferably 24 h per day were based on a non-randomised comparison of two different studies. We hypothesised that oxygen 24 h/day was non-superior to 15 h/day and used the Swedish National Registry for Respiratory Failure (Swedevox) to perform an R-RCT showing that home oxygen 24 h/day does not improve survival, hospitalisation or patient-reported outcomes within 1 year. We describe the entire procedure of REDOX from planning to publication and use it to discuss challenges and potential solutions for future R-RCTs. In summary, common features of R-RCTs are the use of a registry for identification and randomisation of participants and for reporting and collecting baseline and outcome data, and the design is typically used to compare two treatment options. Important strengths are high generalisability, low cost, feasibility for consecutive recruitment in clinical practice, and high completeness of follow-up. Limitations include that coverage, completeness and accuracy of baseline data may differ between registries. Specific challenges (and solutions) in REDOX were addressing an important question (pragmatic clinical trials), management (clinical research support teams), costs (using registry-based infrastructure), different electronic data capture systems (posttrial linkage), slow recruitment (amendment of protocol) and resistance to challenge treatment traditions.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"12 1","pages":"2502237"},"PeriodicalIF":1.4000,"publicationDate":"2025-05-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082728/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2025.2502237","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
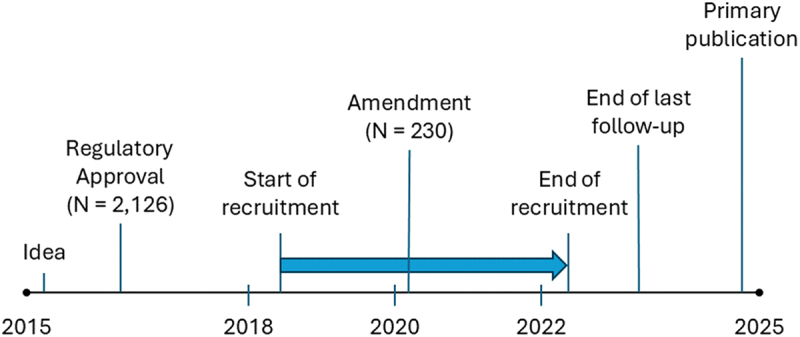
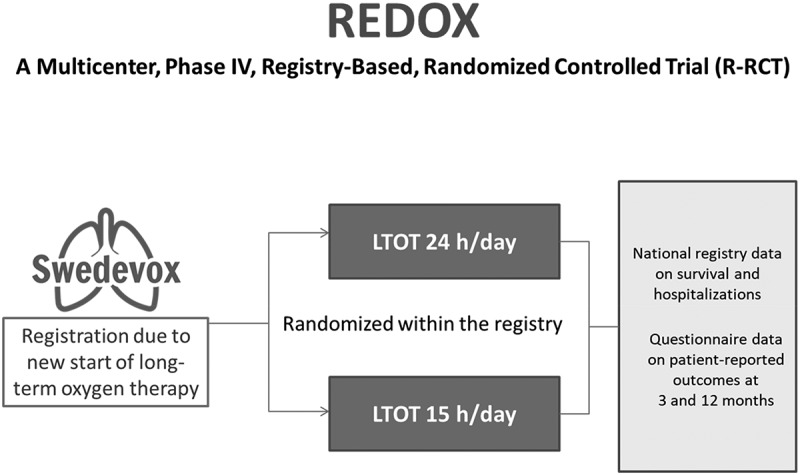
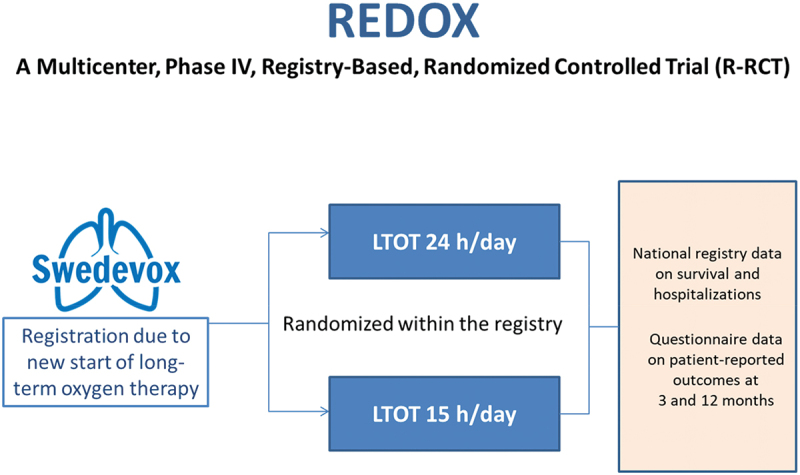
Registry-based randomised controlled trials (R-RCTs) represent a paradigm shift in research, with the potential to accomplish pragmatic but large trials with high external validity. In this paper, we review our experiences from planning and performing the REgistry-based randomised controlled trial of treatment Duration and mortality in long-term OXygen therapy (REDOX) trial, the first R-RCT within respiratory medicine. The REDOX study compared the two established treatment options of home oxygen 15 and 24 h per day. Previous recommendations to use oxygen for at least 15 h but preferably 24 h per day were based on a non-randomised comparison of two different studies. We hypothesised that oxygen 24 h/day was non-superior to 15 h/day and used the Swedish National Registry for Respiratory Failure (Swedevox) to perform an R-RCT showing that home oxygen 24 h/day does not improve survival, hospitalisation or patient-reported outcomes within 1 year. We describe the entire procedure of REDOX from planning to publication and use it to discuss challenges and potential solutions for future R-RCTs. In summary, common features of R-RCTs are the use of a registry for identification and randomisation of participants and for reporting and collecting baseline and outcome data, and the design is typically used to compare two treatment options. Important strengths are high generalisability, low cost, feasibility for consecutive recruitment in clinical practice, and high completeness of follow-up. Limitations include that coverage, completeness and accuracy of baseline data may differ between registries. Specific challenges (and solutions) in REDOX were addressing an important question (pragmatic clinical trials), management (clinical research support teams), costs (using registry-based infrastructure), different electronic data capture systems (posttrial linkage), slow recruitment (amendment of protocol) and resistance to challenge treatment traditions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


