Rudy R Unni, Munir Boodhwani, Ibrahim Jelaidan, David T Harnett, Samia Massalha, Calvin Liang, Graeme Prosperi-Porta, David Glineur, Ian G Burwash, Kwan-Leung Chan, Thais Coutinho, Angel Fu, Nadav Willner, David Messika-Zeitoun, Luc Beauchesne
{"title":"Mechanistic classification of isolated severe aortic regurgitation in a contemporary cohort of patients.","authors":"Rudy R Unni, Munir Boodhwani, Ibrahim Jelaidan, David T Harnett, Samia Massalha, Calvin Liang, Graeme Prosperi-Porta, David Glineur, Ian G Burwash, Kwan-Leung Chan, Thais Coutinho, Angel Fu, Nadav Willner, David Messika-Zeitoun, Luc Beauchesne","doi":"10.1093/ehjopen/oeaf042","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Aortic regurgitation (AR) arises from leaflet disease and/or dilatation of the functional aortic annulus complex. Understanding the mechanisms of AR informs surgical planning of valve and aorta repair. This study investigates the mechanisms, aetiologies, and outcomes of isolated native severe AR in a consecutive cohort of patients.</p><p><strong>Methods and results: </strong>Patients with moderate-to-severe (3+)/severe (4+) native valve AR, identified from our institutional echocardiography database (2014-2018), were included. Exclusions were significant concomitant valve disease, endocarditis, or aortic dissection. AR was classified per the El-Khoury system: Type I (normal leaflet motion: Ia-ascending aorta/sinotubular junction dilatation, Ib-aortic root dilation, Ic-aortic annular dilation), Type II (leaflet prolapse), and Type III (leaflet restriction). Valve anatomy and clinical outcomes, including mortality and surgical intervention, were analyzed. Of 282 patients (77.3% male), 58.5% had multiple AR mechanisms. Type II (leaflet prolapse) was most common (48.6%), followed by Type III (36.2%). Bicuspid aortic valve (BAV) represented 35.5% of the population, with leaflet prolapse observed in 72%. Multiple mechanisms were more frequent in BAV (77% vs. 48%, <i>P</i> < 0.001). After a median follow-up of 4.7 years (available for 97.5% of patients), 158 (57.5%) underwent an intervention with 48.7% having an aortic valve repair or valve-sparing aortic root replacement.</p><p><strong>Conclusion: </strong>Although leaflet prolapse (Type II) was the pre-dominant AR mechanism, multiple contributing mechanisms were often present, particularly in BAV patients. Aortic valve repair accounted for nearly half of surgical interventions, underscoring the importance of mechanism identification to optimize repair and avoid valve replacement.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf042"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076401/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf042","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Aortic regurgitation (AR) arises from leaflet disease and/or dilatation of the functional aortic annulus complex. Understanding the mechanisms of AR informs surgical planning of valve and aorta repair. This study investigates the mechanisms, aetiologies, and outcomes of isolated native severe AR in a consecutive cohort of patients.
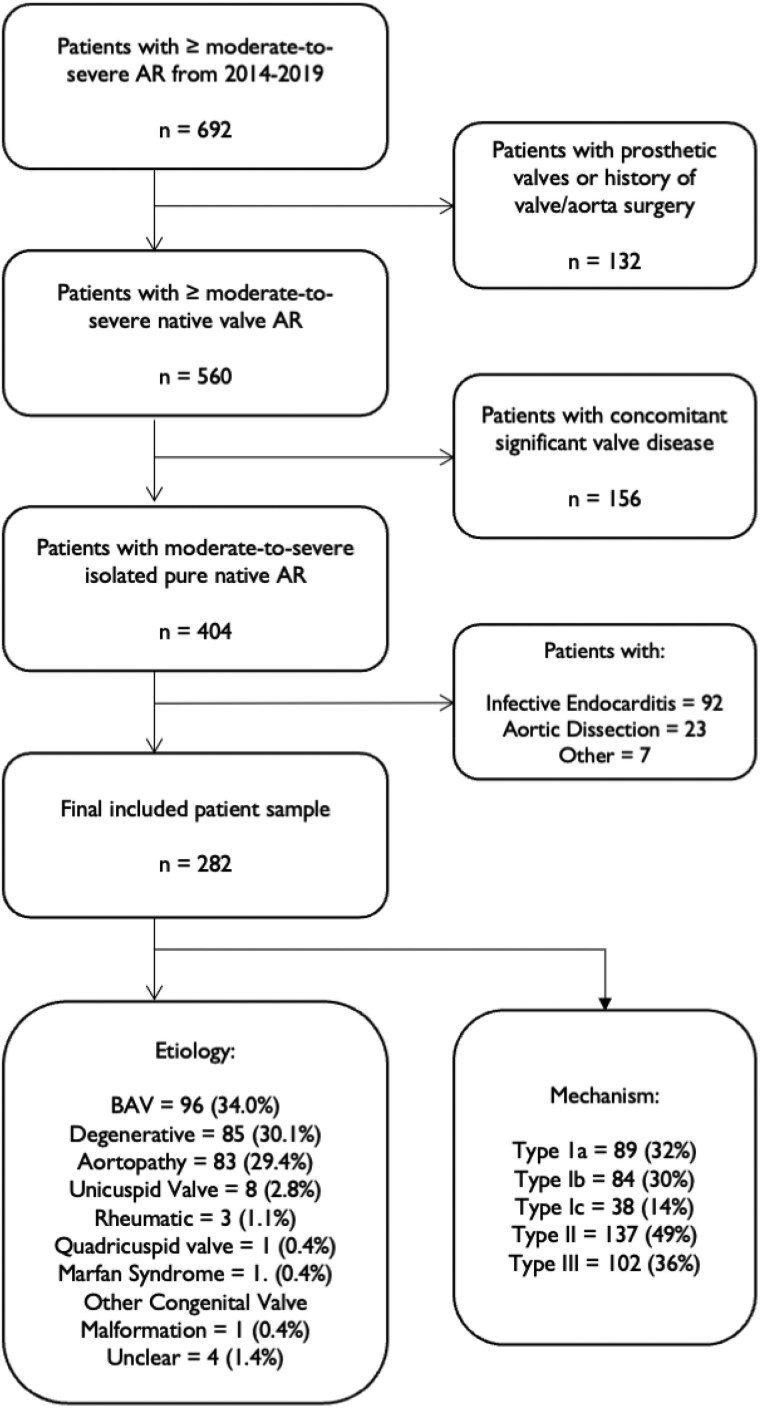
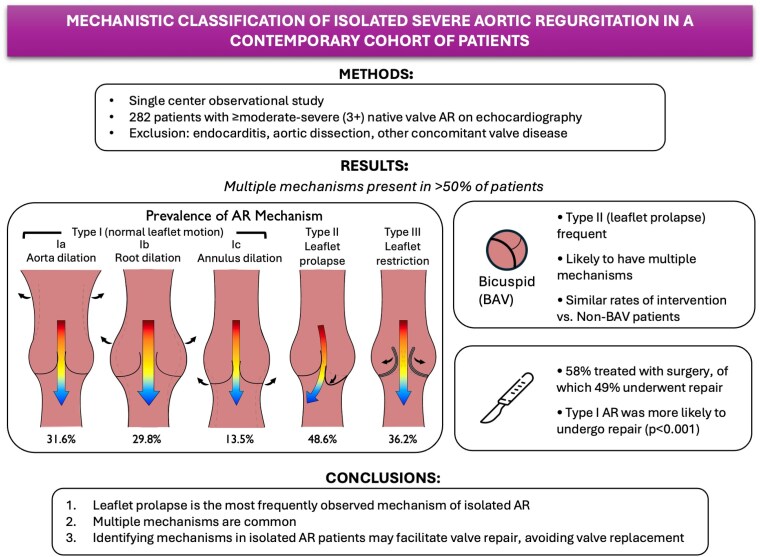
Methods and results: Patients with moderate-to-severe (3+)/severe (4+) native valve AR, identified from our institutional echocardiography database (2014-2018), were included. Exclusions were significant concomitant valve disease, endocarditis, or aortic dissection. AR was classified per the El-Khoury system: Type I (normal leaflet motion: Ia-ascending aorta/sinotubular junction dilatation, Ib-aortic root dilation, Ic-aortic annular dilation), Type II (leaflet prolapse), and Type III (leaflet restriction). Valve anatomy and clinical outcomes, including mortality and surgical intervention, were analyzed. Of 282 patients (77.3% male), 58.5% had multiple AR mechanisms. Type II (leaflet prolapse) was most common (48.6%), followed by Type III (36.2%). Bicuspid aortic valve (BAV) represented 35.5% of the population, with leaflet prolapse observed in 72%. Multiple mechanisms were more frequent in BAV (77% vs. 48%, P < 0.001). After a median follow-up of 4.7 years (available for 97.5% of patients), 158 (57.5%) underwent an intervention with 48.7% having an aortic valve repair or valve-sparing aortic root replacement.
Conclusion: Although leaflet prolapse (Type II) was the pre-dominant AR mechanism, multiple contributing mechanisms were often present, particularly in BAV patients. Aortic valve repair accounted for nearly half of surgical interventions, underscoring the importance of mechanism identification to optimize repair and avoid valve replacement.
目的:主动脉瓣反流(AR)是由小叶疾病和/或功能性主动脉环复合体扩张引起的。了解AR的机制有助于瓣膜和主动脉修复的手术计划。本研究在一组连续的患者中调查了孤立的原生严重AR的机制、病因和结果。方法和结果:纳入了从我们的机构超声心动图数据库(2014-2018)中确定的中度至重度(3+)/重度(4+)原生瓣膜AR患者。排除明显的并发瓣膜疾病、心内膜炎或主动脉夹层。根据El-Khoury系统将AR分为:I型(正常小叶运动:ia -升主动脉/窦小管连接处扩张,ib -主动脉根扩张,ic -主动脉环扩张),II型(小叶脱垂)和III型(小叶受限)。分析瓣膜解剖和临床结果,包括死亡率和手术干预。282例患者(77.3%为男性)中,58.5%存在多种AR机制。II型(小叶脱垂)最常见(48.6%),其次是III型(36.2%)。双尖瓣主动脉瓣(BAV)占人口的35.5%,小叶脱垂占72%。多种机制在BAV中更为常见(77% vs. 48%, P < 0.001)。中位随访时间为4.7年(97.5%的患者可随访),158例(57.5%)患者接受了干预,其中48.7%的患者接受了主动脉瓣修复或保留瓣膜的主动脉根置换术。结论:虽然小叶脱垂(II型)是主要的AR机制,但通常存在多种机制,特别是在BAV患者中。主动脉瓣修复占手术干预的近一半,强调了机制识别对优化修复和避免瓣膜置换术的重要性。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


