Yu Tong Huang, Sofia Addab, Gianluca Bertolizio, Reggie Hamdy, Kelly Thorstad, Argerie Tsimicalis
{"title":"Use of Virtual Reality in the Pediatric Perioperative Setting and for Induction of Anesthesia: Mixed Methods Pilot Feasibility Study.","authors":"Yu Tong Huang, Sofia Addab, Gianluca Bertolizio, Reggie Hamdy, Kelly Thorstad, Argerie Tsimicalis","doi":"10.2196/58905","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Children commonly experience high levels of anxiety prior to surgery. This distress is associated with postoperative maladaptive behaviors. Virtual reality (VR) is an innovative tool for reducing anxiety and pain during various medical procedures. Previous randomized controlled trials have demonstrated its efficacy in reducing children's anxiety in the preoperative waiting room or during induction.</p><p><strong>Objective: </strong>The primary aim of this study was to examine the feasibility of VR distraction throughout the perioperative period, from the waiting room until the induction of general anesthesia (GA). Secondary aims were to assess its clinical utility, tolerability, and initial clinical efficacy.</p><p><strong>Methods: </strong>A mixed methods, concurrent triangulation feasibility trial was piloted at the Shriners Hospitals for Children-Canada. Participants played an interactive VR game throughout the perioperative period, starting from the waiting room until induction. Feasibility was examined with the duration of the VR intervention, recording the number of interruptions, and taking field notes. Clinical utility was assessed using a perception questionnaire. Tolerability was evaluated by the Child Simulator Sickness Questionnaire (CSSQ). Initial clinical efficacy was assessed by the Faces Pain Scale-Revised, Faces Anxiety Scale, Graphic Rating Scale for multidimensional pain, the Induction Compliance Checklist, and the Pediatric Anesthesia Emergence Delirium scale. Quantitative data were supported with field notes and semistructured interviews with patients and parents. Quantitative and qualitative themes were compared via the triangulation protocol to produce final themes.</p><p><strong>Results: </strong>A total of 39 patients, with a mean age of 11.9 (SD 2.8) years, undergoing elective surgery under GA participated in the study. Stakeholders, including patients, parents, and health care providers, were receptive and willing to adapt to VR. Of the 39 patients, 19 (49%) continued to use VR during transportation and 6 (15%) were induced with VR. Barriers to feasibility included (1) interruptions to VR in 92% (36/39) of patients by health care professionals, (2) unpredictable surgery delays prolonging the duration of the VR intervention (mean 23.1, SD 24.4 minutes; range 5-150 minutes), and (3) discontinuation of VR before induction due to mask seal (n=3) and discomfort with supine positioning (n=2). Patients were generally satisfied with VR, deemed it acceptable and easy to use, and would recommend it to others. VR was tolerable with no self-reported simulator sickness (CSSQ: mean 0.01, SD 0.1). The mean Faces Anxiety Score was 1.5 (SD 1.1) at baseline and 0.7 (SD 0.9) during VR.</p><p><strong>Conclusions: </strong>While VR demonstrated good clinical utility and was well tolerated in the broad perioperative setting, this study highlighted important feasibility barriers in the waiting room and especially during induction of anesthesia, both at the organizational and technical levels. This study highlights several considerations that should be carefully addressed for the successful implementation of perioperative VR.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"8 ","pages":"e58905"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101790/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/58905","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Children commonly experience high levels of anxiety prior to surgery. This distress is associated with postoperative maladaptive behaviors. Virtual reality (VR) is an innovative tool for reducing anxiety and pain during various medical procedures. Previous randomized controlled trials have demonstrated its efficacy in reducing children's anxiety in the preoperative waiting room or during induction.
Objective: The primary aim of this study was to examine the feasibility of VR distraction throughout the perioperative period, from the waiting room until the induction of general anesthesia (GA). Secondary aims were to assess its clinical utility, tolerability, and initial clinical efficacy.
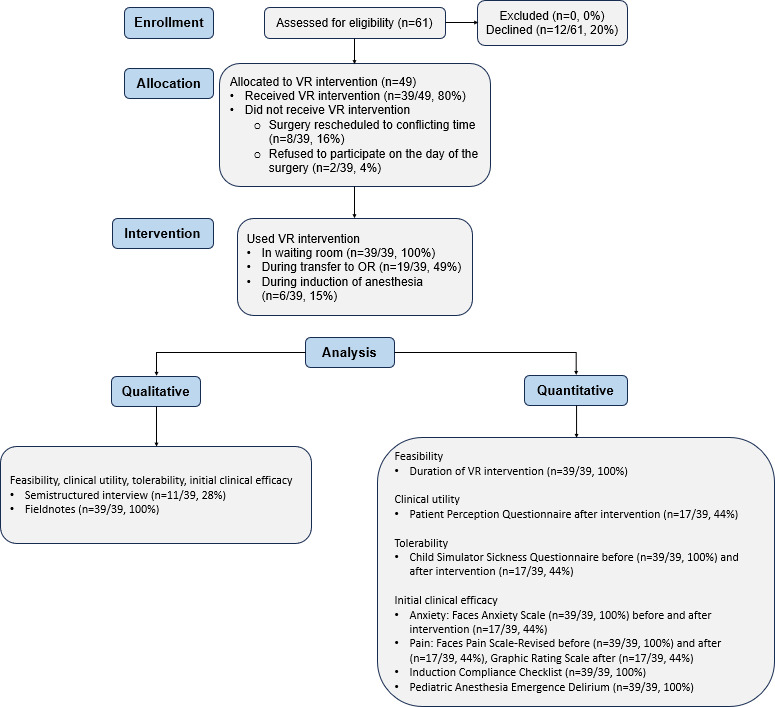
Methods: A mixed methods, concurrent triangulation feasibility trial was piloted at the Shriners Hospitals for Children-Canada. Participants played an interactive VR game throughout the perioperative period, starting from the waiting room until induction. Feasibility was examined with the duration of the VR intervention, recording the number of interruptions, and taking field notes. Clinical utility was assessed using a perception questionnaire. Tolerability was evaluated by the Child Simulator Sickness Questionnaire (CSSQ). Initial clinical efficacy was assessed by the Faces Pain Scale-Revised, Faces Anxiety Scale, Graphic Rating Scale for multidimensional pain, the Induction Compliance Checklist, and the Pediatric Anesthesia Emergence Delirium scale. Quantitative data were supported with field notes and semistructured interviews with patients and parents. Quantitative and qualitative themes were compared via the triangulation protocol to produce final themes.
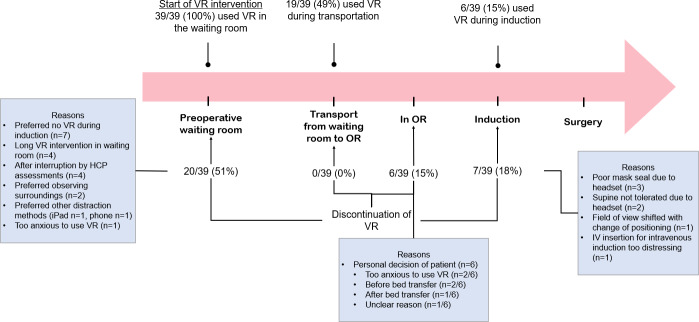
Results: A total of 39 patients, with a mean age of 11.9 (SD 2.8) years, undergoing elective surgery under GA participated in the study. Stakeholders, including patients, parents, and health care providers, were receptive and willing to adapt to VR. Of the 39 patients, 19 (49%) continued to use VR during transportation and 6 (15%) were induced with VR. Barriers to feasibility included (1) interruptions to VR in 92% (36/39) of patients by health care professionals, (2) unpredictable surgery delays prolonging the duration of the VR intervention (mean 23.1, SD 24.4 minutes; range 5-150 minutes), and (3) discontinuation of VR before induction due to mask seal (n=3) and discomfort with supine positioning (n=2). Patients were generally satisfied with VR, deemed it acceptable and easy to use, and would recommend it to others. VR was tolerable with no self-reported simulator sickness (CSSQ: mean 0.01, SD 0.1). The mean Faces Anxiety Score was 1.5 (SD 1.1) at baseline and 0.7 (SD 0.9) during VR.
Conclusions: While VR demonstrated good clinical utility and was well tolerated in the broad perioperative setting, this study highlighted important feasibility barriers in the waiting room and especially during induction of anesthesia, both at the organizational and technical levels. This study highlights several considerations that should be carefully addressed for the successful implementation of perioperative VR.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


