Arturo M Ruiz-Beltrán, Gerardo Chacón-Loyola, Ricardo L Barajas-Campos, Alejandro Alcaraz-Guzmán, Manuel A Montoya-Hernández, Leonardo D Alcázar-Flores, Laura L Rodríguez-Chávez
{"title":"Performance of scoring systems for predicting mortality after cardiac surgery in the elderly.","authors":"Arturo M Ruiz-Beltrán, Gerardo Chacón-Loyola, Ricardo L Barajas-Campos, Alejandro Alcaraz-Guzmán, Manuel A Montoya-Hernández, Leonardo D Alcázar-Flores, Laura L Rodríguez-Chávez","doi":"10.47487/apcyccv.v6i1.459","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the predictive ability of traditional risk scores and frailty assessment for 30-day mortality in elderly patients undergoing cardiac surgery.</p><p><strong>Materials and methods: </strong>A single-center retrospective cohort study was conducted, including elderly patients (≥75 years old) who underwent cardiac surgery between January 2005 and December 2015. EuroSCORE II, STS (Society of Thoracic Surgeons) score, Charlson Comorbidity Index, and Electronic Frailty Index scores were calculated to assess their predictive ability for 30-day mortality using receiver operating characteristic (ROC) curves and corresponding areas under the curve (AUC).</p><p><strong>Results: </strong>A total of 203 patients were included during the study period, of whom 33% underwent isolated coronary bypass surgery. The overall 30-day mortality rate was 17.6%. Patients who died within the first 30 days exhibited higher scores on EuroSCORE II, STS, and the Electronic Frailty Index. The areas under the ROC curves were: EuroSCORE II, 0.74 (95% CI: 0.66-0.81); STS, 0.66 (95% CI: 0.57-0.77); Charlson Comorbidity Index, 0.60 (95% CI: 0.49-0.70); and Electronic Frailty Index, 0.63 (95% CI: 0.52-0.73).</p><p><strong>Conclusions: </strong>In this cohort of elderly patients undergoing cardiac surgery, EuroSCORE II demonstrated the best performance in predicting 30-day mortality.</p>","PeriodicalId":72295,"journal":{"name":"Archivos Peruanos de cardiologia y cirugia cardiovascular","volume":"6 1","pages":"29-35"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076771/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archivos Peruanos de cardiologia y cirugia cardiovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.47487/apcyccv.v6i1.459","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate the predictive ability of traditional risk scores and frailty assessment for 30-day mortality in elderly patients undergoing cardiac surgery.
Materials and methods: A single-center retrospective cohort study was conducted, including elderly patients (≥75 years old) who underwent cardiac surgery between January 2005 and December 2015. EuroSCORE II, STS (Society of Thoracic Surgeons) score, Charlson Comorbidity Index, and Electronic Frailty Index scores were calculated to assess their predictive ability for 30-day mortality using receiver operating characteristic (ROC) curves and corresponding areas under the curve (AUC).
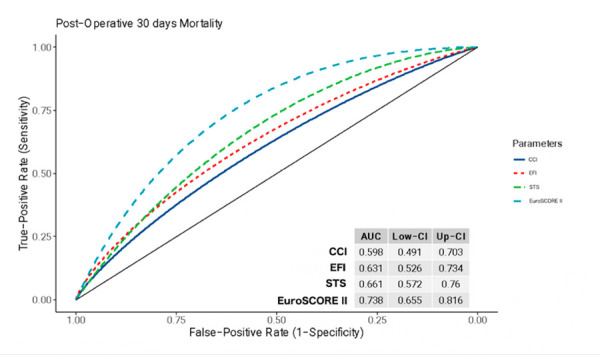
Results: A total of 203 patients were included during the study period, of whom 33% underwent isolated coronary bypass surgery. The overall 30-day mortality rate was 17.6%. Patients who died within the first 30 days exhibited higher scores on EuroSCORE II, STS, and the Electronic Frailty Index. The areas under the ROC curves were: EuroSCORE II, 0.74 (95% CI: 0.66-0.81); STS, 0.66 (95% CI: 0.57-0.77); Charlson Comorbidity Index, 0.60 (95% CI: 0.49-0.70); and Electronic Frailty Index, 0.63 (95% CI: 0.52-0.73).
Conclusions: In this cohort of elderly patients undergoing cardiac surgery, EuroSCORE II demonstrated the best performance in predicting 30-day mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


