{"title":"Enhancing Lung Function in Novice Athletes: The Role of Respiratory Muscle Training.","authors":"Thiagarajan Subramanian, Manu Goyal","doi":"10.15280/jlm.2025.15.1.31","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Respiratory muscle training (RMT) plays a vital role in improving respiratory muscle strength, mitigating inspiratory muscle fatigue, and influencing the metaboreflex mechanism, thereby enhancing cardiorespiratory endurance during sports. Performing endurance activities and using devices that improve lung function can delay inspiratory muscle fatigue and improve total sports performance. The aim of this study was to determine the effect of use of newly developed RMT devices under the golden ratio principle with conventional training on lung function enhancement in novice athletes, as well as compare a new RMT with conventional (CON) treatment.</p><p><strong>Methods: </strong>This study included 12 participants who were allocated randomly to either the RMT or CON group (n = 6 each). Both groups were trained for 15 minutes daily for four weeks. Both groups were initially tested for respiratory pressures and capacities maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), forced expiratory volume in first second (FEV1), forced vital capacity (FVC), and FEV1/FVC at baseline and post-intervention. Within-group and between-group comparisons were performed using paired t-tests and independent t-tests, respectively.</p><p><strong>Results: </strong>The respiratory pressures of the RMT group after training (pre-RMT 425.00 ± 277.04 mmWC vs. post-RMT 541.67 ± 274.62 mmWC) were significantly improved (t = 11.07, p < 0.001) compared with those of the CON treatment group (pre-RMT 508.33 ± 217.75 mmWC vs. post-RMT 575.00 ± 229.67 mmWC). The new RMT device improved MIP, MEP, and lung function, with greater gains in FEV1 (pre-RMT 2.66 ± 0.74 L vs. post-RMT 2.86 ± 0.70 L) (pre-CON 3.04 ± 0.80 L vs. post-CON 3.06 ± 0.74 L), FVC (pre-RMT 3.03 ± 0.99 L vs. post-RMT 3.22 ± 0.94 L) (pre-CON 3.33 ± 1.06 L vs. post-CON 3.29 ± 0.99 L), and the FEV1/FVC ratio compared with both the RMT and CON treatment groups. Although the between-group differences in MIP and MEP were not statistically significant, improvements in FEV1 and FVC were significantly higher in the new RMT group than in the CON treatment group (p < 0.05).</p><p><strong>Conclusion: </strong>The findings revealed that the RMT devices helped to improve respiratory pressures and capacities to enhance endurance among novice athletes. Furthermore, this golden ratio-designed device was found to help improve lung performance.</p>","PeriodicalId":73805,"journal":{"name":"Journal of lifestyle medicine","volume":"15 1","pages":"31-37"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076046/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of lifestyle medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15280/jlm.2025.15.1.31","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Respiratory muscle training (RMT) plays a vital role in improving respiratory muscle strength, mitigating inspiratory muscle fatigue, and influencing the metaboreflex mechanism, thereby enhancing cardiorespiratory endurance during sports. Performing endurance activities and using devices that improve lung function can delay inspiratory muscle fatigue and improve total sports performance. The aim of this study was to determine the effect of use of newly developed RMT devices under the golden ratio principle with conventional training on lung function enhancement in novice athletes, as well as compare a new RMT with conventional (CON) treatment.
Methods: This study included 12 participants who were allocated randomly to either the RMT or CON group (n = 6 each). Both groups were trained for 15 minutes daily for four weeks. Both groups were initially tested for respiratory pressures and capacities maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), forced expiratory volume in first second (FEV1), forced vital capacity (FVC), and FEV1/FVC at baseline and post-intervention. Within-group and between-group comparisons were performed using paired t-tests and independent t-tests, respectively.
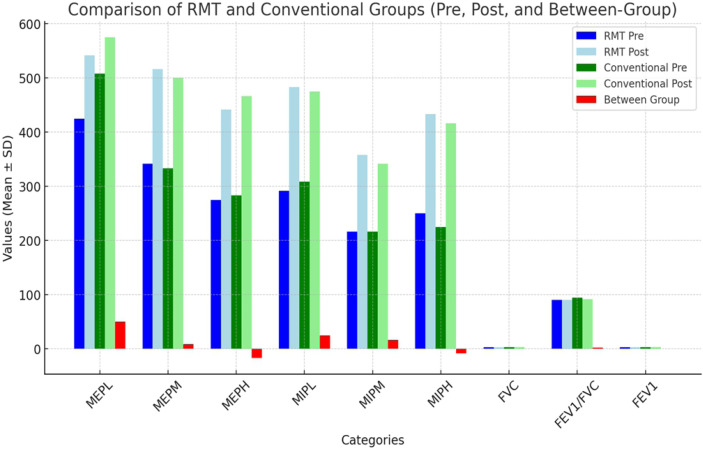
Results: The respiratory pressures of the RMT group after training (pre-RMT 425.00 ± 277.04 mmWC vs. post-RMT 541.67 ± 274.62 mmWC) were significantly improved (t = 11.07, p < 0.001) compared with those of the CON treatment group (pre-RMT 508.33 ± 217.75 mmWC vs. post-RMT 575.00 ± 229.67 mmWC). The new RMT device improved MIP, MEP, and lung function, with greater gains in FEV1 (pre-RMT 2.66 ± 0.74 L vs. post-RMT 2.86 ± 0.70 L) (pre-CON 3.04 ± 0.80 L vs. post-CON 3.06 ± 0.74 L), FVC (pre-RMT 3.03 ± 0.99 L vs. post-RMT 3.22 ± 0.94 L) (pre-CON 3.33 ± 1.06 L vs. post-CON 3.29 ± 0.99 L), and the FEV1/FVC ratio compared with both the RMT and CON treatment groups. Although the between-group differences in MIP and MEP were not statistically significant, improvements in FEV1 and FVC were significantly higher in the new RMT group than in the CON treatment group (p < 0.05).
Conclusion: The findings revealed that the RMT devices helped to improve respiratory pressures and capacities to enhance endurance among novice athletes. Furthermore, this golden ratio-designed device was found to help improve lung performance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


