{"title":"Delayed Diagnosis and Outcomes in Acute Aortic Dissection: A 10-Year Single-Center Retrospective Study.","authors":"Suluck Kanoksirirat, Adisak Nithimathachoke","doi":"10.2147/OAEM.S496279","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute aortic dissection is a rare and life-threatening condition with highly variable clinical presentations, often resulting in atypical symptoms and initial misdiagnosis. This study aimed to investigate clinical presentations and explore the associations between clinical characteristics, delayed diagnosis, and in-hospital mortality among patients with acute aortic dissection.</p><p><strong>Methods: </strong>A retrospective chart review was performed on patients presenting with acute aortic dissection at an urban academic emergency department in Thailand between January 1, 2011, and December 31, 2020. Baseline characteristics, clinical presentations, imaging findings, delayed diagnosis (>4 h from first emergency department contact), and in-hospital mortality rates were analyzed.</p><p><strong>Results: </strong>The study included 103 patient charts, predominately men (71 patients), with a median age of 71 years (interquartile range of 58-78 years). Abdominal pain (36.9%) and thoracic pain (24.3%) were the most common presenting symptoms. Dyspnea (11.7%), altered consciousness (4.9%), and syncope (4.9%) were the three main painless presenting atypical symptoms. Atypical presentations were not significantly associated with delayed diagnosis, which occurred in 27.2% of cases. Normotension, a history of coronary artery disease, and pleural effusion were associated with delayed diagnosis. Abnormal chest films were major risk factors for in-hospital mortality, observed in 22.3% of patients with acute aortic dissection, whereas delayed diagnosis was not directly related to such mortality.</p><p><strong>Conclusion: </strong>The incidence of acute aortic dissection in the urban Thai population was 32.4 per 100,000 patient-years, with a range of clinical presentations. A high index of suspicion for AAD is crucial for timely diagnosis, even in patients with atypical symptoms and seemingly normal vital signs. Careful interpretation of chest radiographs is essential as abnormal chest X-ray findings are associated with a poorer prognosis.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"17 ","pages":"173-183"},"PeriodicalIF":1.5000,"publicationDate":"2025-05-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12075430/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S496279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Acute aortic dissection is a rare and life-threatening condition with highly variable clinical presentations, often resulting in atypical symptoms and initial misdiagnosis. This study aimed to investigate clinical presentations and explore the associations between clinical characteristics, delayed diagnosis, and in-hospital mortality among patients with acute aortic dissection.
Methods: A retrospective chart review was performed on patients presenting with acute aortic dissection at an urban academic emergency department in Thailand between January 1, 2011, and December 31, 2020. Baseline characteristics, clinical presentations, imaging findings, delayed diagnosis (>4 h from first emergency department contact), and in-hospital mortality rates were analyzed.
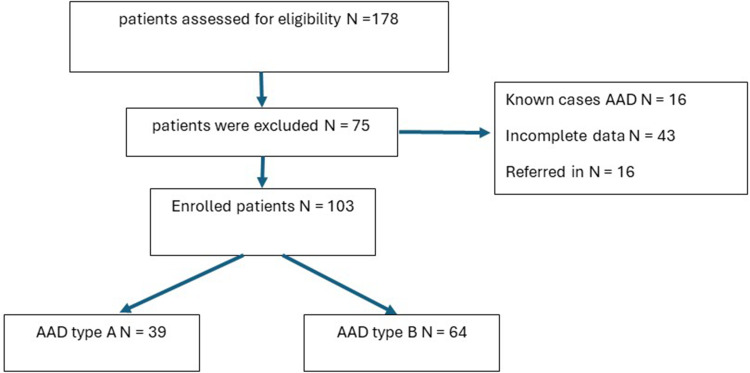
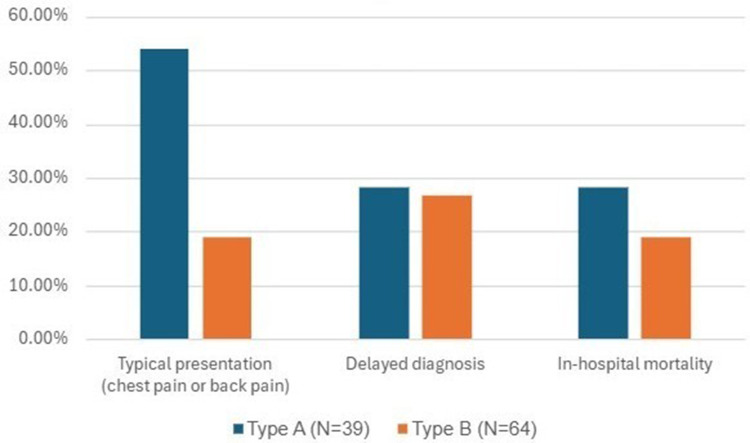
Results: The study included 103 patient charts, predominately men (71 patients), with a median age of 71 years (interquartile range of 58-78 years). Abdominal pain (36.9%) and thoracic pain (24.3%) were the most common presenting symptoms. Dyspnea (11.7%), altered consciousness (4.9%), and syncope (4.9%) were the three main painless presenting atypical symptoms. Atypical presentations were not significantly associated with delayed diagnosis, which occurred in 27.2% of cases. Normotension, a history of coronary artery disease, and pleural effusion were associated with delayed diagnosis. Abnormal chest films were major risk factors for in-hospital mortality, observed in 22.3% of patients with acute aortic dissection, whereas delayed diagnosis was not directly related to such mortality.
Conclusion: The incidence of acute aortic dissection in the urban Thai population was 32.4 per 100,000 patient-years, with a range of clinical presentations. A high index of suspicion for AAD is crucial for timely diagnosis, even in patients with atypical symptoms and seemingly normal vital signs. Careful interpretation of chest radiographs is essential as abnormal chest X-ray findings are associated with a poorer prognosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


