Raffaele Vitiello, Elisa Pesare, Giacomo Capece, Emidio Di Gialleonardo, Andrea De Matthaeis, Francesco Franceschi, Giulio Maccauro, Marcello Covino
{"title":"Surgical timing and clinical factor predicting in-hospital mortality in older adults with hip fractures: a neuronal network analysis.","authors":"Raffaele Vitiello, Elisa Pesare, Giacomo Capece, Emidio Di Gialleonardo, Andrea De Matthaeis, Francesco Franceschi, Giulio Maccauro, Marcello Covino","doi":"10.1186/s10195-025-00846-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hip fractures in older adults are associated with a significant mortality rate, which has been reported to be around 35% within a year. Today, the incidence of these fractures is on the rise, and this trend is expected to increase even more owing to the aging of the population. Treatment timing and perioperative management of these patients are typically challenging owing to the presence of multiple comorbidities that are important risk factors for mortality after surgery. This study aims to evaluate the relationship between surgical timing and in-hospital mortality, analyzing the role of both acute events and chronic preexisting comorbidities in patient outcomes.</p><p><strong>Materials and methods: </strong>This is a single-center, retrospective observational study (from January 2018 until June 2023). All consecutive patients ≥ 65 years with a diagnosis of proximal femur fracture were enrolled. The primary study endpoint was to evaluate risk factors associated with in-hospital mortality. The secondary endpoint was the assessment of the relationship between surgical timing and in-hospital mortality, including factors such as preexisting comorbidities, the Charlson Comorbidity Index, and the Nottingham Hip Fracture Score. The relative weight of each factor for predicting the mortality rate was also evaluated using neural network analysis, comparing patients treated within 24 h to those treated after a longer surgical delay.</p><p><strong>Results: </strong>Among the 2320 patients enrolled, 1391 (60%) underwent surgery within 24 h, while 929 patients (40%) were treated after 24 h. For patients who underwent surgery within 24 h, the in-hospital mortality was 2.8%, and for those who underwent surgery after 24 h, it was 5.2% (p = 0.046; odds ratio (OR) 1.58). Age (p = 0.001; OR 1.06) and Nottingham score (p = 0.04; OR 1.32) are factors predicting mortality. Acute infections were related to a high risk of mortality (p = 0.001; OR 5.99), both in patients treated within and after 24 h. Acute events, such as atrial fibrillation and electrolyte imbalance, were related to mortality risk only in patients treated within 24 h (p = 0.001 versus p = 0.51). Neural network analysis revealed that atrial fibrillation (AF), flutter, and electrolyte imbalance had the highest relative weight for mortality in patients treated in the first 24 h; by contrast, renal failure and pneumonia were most present in patients who died that were treated after 24 h.</p><p><strong>Conclusions: </strong>Hip fracture is known to be a significant cause of morbidity and mortality in older adults. The impact of the timing of surgical treatment in those patients is crucial for postoperative outcomes. Early surgery is essential to reduce the risk of mortality. Our study has shown that, while in the case of acute and reversible conditions, waiting about 24 h to stabilize the patient with preoperative stabilization protocols, such as managing anticoagulation, optimizing hemodynamics, or addressing acute medical conditions including infection prevention, guarantees better results, in the case of sepsis or acute infection presence, the prolonged waiting to optimize patients before and after surgery does not help improve outcomes.</p>","PeriodicalId":48603,"journal":{"name":"Journal of Orthopaedics and Traumatology","volume":"26 1","pages":"30"},"PeriodicalIF":3.7000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12078743/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedics and Traumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s10195-025-00846-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Hip fractures in older adults are associated with a significant mortality rate, which has been reported to be around 35% within a year. Today, the incidence of these fractures is on the rise, and this trend is expected to increase even more owing to the aging of the population. Treatment timing and perioperative management of these patients are typically challenging owing to the presence of multiple comorbidities that are important risk factors for mortality after surgery. This study aims to evaluate the relationship between surgical timing and in-hospital mortality, analyzing the role of both acute events and chronic preexisting comorbidities in patient outcomes.
Materials and methods: This is a single-center, retrospective observational study (from January 2018 until June 2023). All consecutive patients ≥ 65 years with a diagnosis of proximal femur fracture were enrolled. The primary study endpoint was to evaluate risk factors associated with in-hospital mortality. The secondary endpoint was the assessment of the relationship between surgical timing and in-hospital mortality, including factors such as preexisting comorbidities, the Charlson Comorbidity Index, and the Nottingham Hip Fracture Score. The relative weight of each factor for predicting the mortality rate was also evaluated using neural network analysis, comparing patients treated within 24 h to those treated after a longer surgical delay.
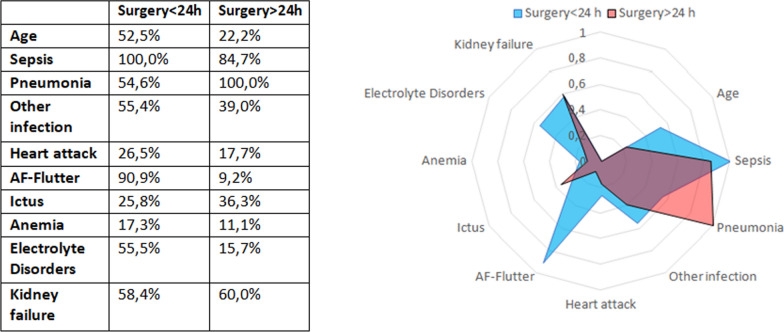
Results: Among the 2320 patients enrolled, 1391 (60%) underwent surgery within 24 h, while 929 patients (40%) were treated after 24 h. For patients who underwent surgery within 24 h, the in-hospital mortality was 2.8%, and for those who underwent surgery after 24 h, it was 5.2% (p = 0.046; odds ratio (OR) 1.58). Age (p = 0.001; OR 1.06) and Nottingham score (p = 0.04; OR 1.32) are factors predicting mortality. Acute infections were related to a high risk of mortality (p = 0.001; OR 5.99), both in patients treated within and after 24 h. Acute events, such as atrial fibrillation and electrolyte imbalance, were related to mortality risk only in patients treated within 24 h (p = 0.001 versus p = 0.51). Neural network analysis revealed that atrial fibrillation (AF), flutter, and electrolyte imbalance had the highest relative weight for mortality in patients treated in the first 24 h; by contrast, renal failure and pneumonia were most present in patients who died that were treated after 24 h.
Conclusions: Hip fracture is known to be a significant cause of morbidity and mortality in older adults. The impact of the timing of surgical treatment in those patients is crucial for postoperative outcomes. Early surgery is essential to reduce the risk of mortality. Our study has shown that, while in the case of acute and reversible conditions, waiting about 24 h to stabilize the patient with preoperative stabilization protocols, such as managing anticoagulation, optimizing hemodynamics, or addressing acute medical conditions including infection prevention, guarantees better results, in the case of sepsis or acute infection presence, the prolonged waiting to optimize patients before and after surgery does not help improve outcomes.
期刊介绍:
The Journal of Orthopaedics and Traumatology, the official open access peer-reviewed journal of the Italian Society of Orthopaedics and Traumatology, publishes original papers reporting basic or clinical research in the field of orthopaedic and traumatologic surgery, as well as systematic reviews, brief communications, case reports and letters to the Editor. Narrative instructional reviews and commentaries to original articles may be commissioned by Editors from eminent colleagues. The Journal of Orthopaedics and Traumatology aims to be an international forum for the communication and exchange of ideas concerning the various aspects of orthopaedics and musculoskeletal trauma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


