Louie Cao, Gloria J Hong, Michael Abiragi, Jonathan Le, P Ryan Tacon, I-Min Chiu, Jignesh Patel, Lily K Stern, Chathuri Daluwatte, David Ouyang, Piero Ricchiuto
{"title":"Ratio of interventricular septal thickness to global longitudinal strain accurately identifies cardiac amyloidosis.","authors":"Louie Cao, Gloria J Hong, Michael Abiragi, Jonathan Le, P Ryan Tacon, I-Min Chiu, Jignesh Patel, Lily K Stern, Chathuri Daluwatte, David Ouyang, Piero Ricchiuto","doi":"10.1136/openhrt-2024-003120","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Conventional transthoracic echocardiographic measurements like global longitudinal strain (GLS) have shown promise in distinguishing cardiac amyloidosis (CA), but with limited specificity. We investigated the performance of common echo measurements, GLS, and their combinations in discriminating CA from an undifferentiated cohort with increased left ventricular wall thickness.</p><p><strong>Methods: </strong>We conducted a retrospective single-centre case-control study of 876 echos from 232 patients with CA and 1325 echos from 279 patients who underwent pyrophosphate scintigraphy but had CA definitively ruled out. Common echo measurements were collected and additional GLS measurements were performed post hoc. We reported discrimination performance with the area under the receiver operating characteristic curve (AUC) and associated sensitivity, specificity and positive predictive value at the optimal threshold.</p><p><strong>Results: </strong>We found that the ratio of end-diastolic interventricular septal thickness (IVSd) to GLS had the highest performance in differentiating CA with an AUC of 0.812. At the optimal threshold of >0.15, IVSd/GLS had a sensitivity of 0.70 and specificity of 0.80 for CA. Other measurements and ratios, including the ratio of left ventricular ejection fraction to GLS (AUC 0.682), had lower performance when evaluated against a suspicious control cohort with increased left ventricular wall thickness.</p><p><strong>Conclusion: </strong>If validated in prospective multi-centre studies, the routine measurement of IVSd/GLS can assist with earlier diagnosis of CA, resulting in earlier initiation of treatment in this underserved population.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12083331/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2024-003120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Conventional transthoracic echocardiographic measurements like global longitudinal strain (GLS) have shown promise in distinguishing cardiac amyloidosis (CA), but with limited specificity. We investigated the performance of common echo measurements, GLS, and their combinations in discriminating CA from an undifferentiated cohort with increased left ventricular wall thickness.
Methods: We conducted a retrospective single-centre case-control study of 876 echos from 232 patients with CA and 1325 echos from 279 patients who underwent pyrophosphate scintigraphy but had CA definitively ruled out. Common echo measurements were collected and additional GLS measurements were performed post hoc. We reported discrimination performance with the area under the receiver operating characteristic curve (AUC) and associated sensitivity, specificity and positive predictive value at the optimal threshold.
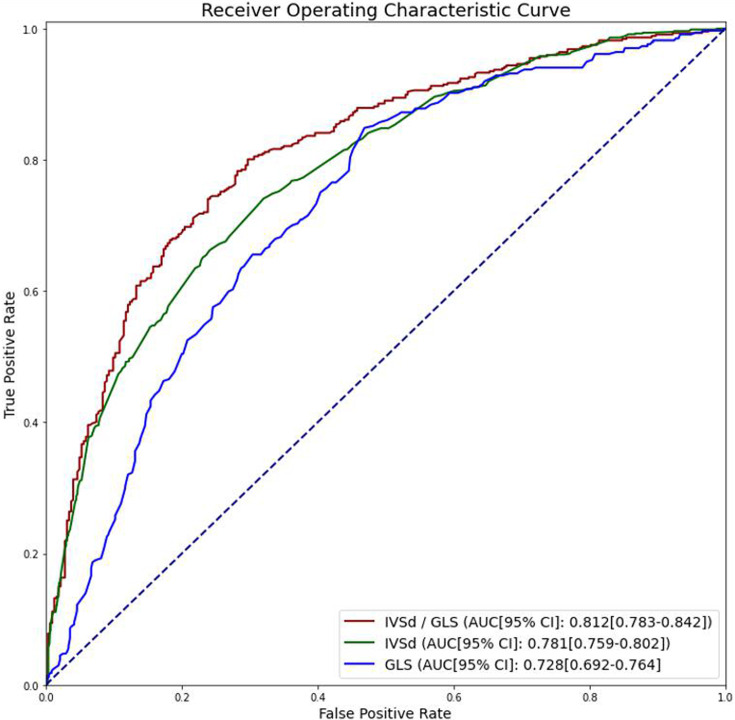
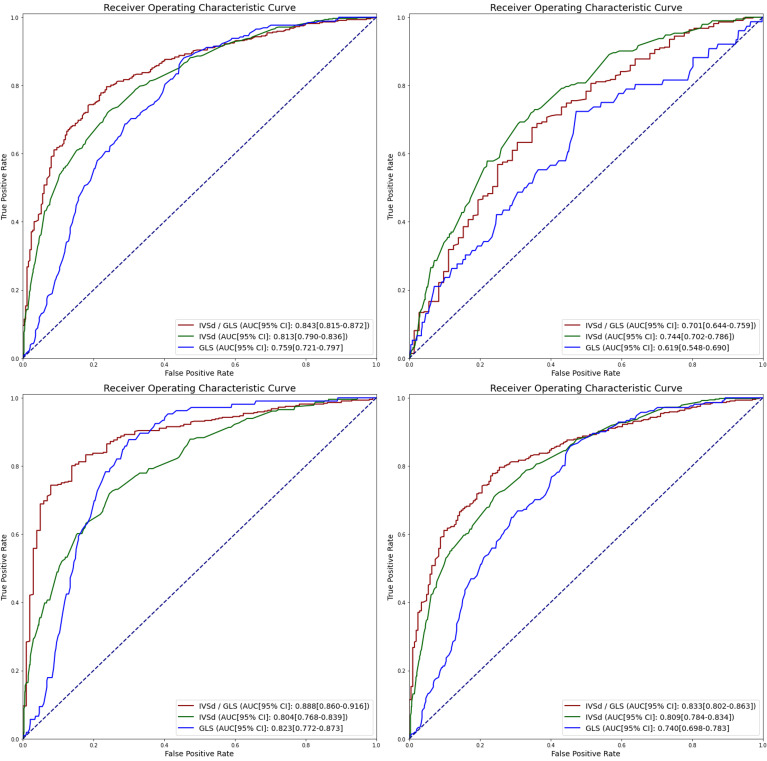
Results: We found that the ratio of end-diastolic interventricular septal thickness (IVSd) to GLS had the highest performance in differentiating CA with an AUC of 0.812. At the optimal threshold of >0.15, IVSd/GLS had a sensitivity of 0.70 and specificity of 0.80 for CA. Other measurements and ratios, including the ratio of left ventricular ejection fraction to GLS (AUC 0.682), had lower performance when evaluated against a suspicious control cohort with increased left ventricular wall thickness.
Conclusion: If validated in prospective multi-centre studies, the routine measurement of IVSd/GLS can assist with earlier diagnosis of CA, resulting in earlier initiation of treatment in this underserved population.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


