Reducing inappropriate antibiotic use in febrile neutropenia in hematology patients through the implementation of an antibiotic de-escalation protocol.
Jinghao Nicholas Ngiam, Victor Ling, Matthew Chung Yi Koh, Mohamed Nasar Fathima Rofina Farveen, Shi Hui Clarice Choong, Li Mei Michelle Poon, Liang Piu Koh, Nares Smitasin, Lionel Hon-Wai Lum
{"title":"Reducing inappropriate antibiotic use in febrile neutropenia in hematology patients through the implementation of an antibiotic de-escalation protocol.","authors":"Jinghao Nicholas Ngiam, Victor Ling, Matthew Chung Yi Koh, Mohamed Nasar Fathima Rofina Farveen, Shi Hui Clarice Choong, Li Mei Michelle Poon, Liang Piu Koh, Nares Smitasin, Lionel Hon-Wai Lum","doi":"10.1017/ice.2025.90","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Broad-spectrum antibiotic use in febrile neutropenia is often driven by concerns for severe and drug-resistant infections. In select patients who do not have an active infection and improve, their prolonged and unnecessary use contributes to antimicrobial resistance, drug toxicity, and increased healthcare costs. We describe the implementation of an antibiotic de-escalation protocol to reduce inappropriate antibiotic use in febrile neutropenia among hematology patients.</p><p><strong>Methods: </strong>We conducted baseline analysis (January-June 2024) of antibiotic use in febrile neutropenia cases admitted under hematology. Interventions included the (i) development of an antibiotic de-escalation protocol to guide clinical management, (ii) a roadshow to educate and improve uptake of this protocol, and (iii) regular feedback via \"report cards\" for hematology teams. The primary outcome was the proportion of febrile neutropenia cases with inappropriate antibiotic use, with secondary measures including adverse outcomes (in-hospital mortality, <i>Clostridioides difficile</i> infection, need for intensive care).</p><p><strong>Results: </strong>Baseline data indicated inappropriate antibiotic use rates of 45.5-66.7% per month from January to June 2024, with 13-28 days of inappropriate therapy. The protocol was developed in July 2024, with a subsequent roadshow to promote its uptake. Regular feedback was provided in the form of \"report cards\" every 2-monthly thereafter. Post-intervention, inappropriate antibiotic use decreased to a median of 23.35% from July to December 2024, with no observed increase in adverse outcomes.</p><p><strong>Conclusions: </strong>The implementation of a structured de-escalation protocol, combined with frequent education and feedback, effectively reduced inappropriate antibiotic use in febrile neutropenia without compromising patient safety.</p>","PeriodicalId":13663,"journal":{"name":"Infection Control and Hospital Epidemiology","volume":" ","pages":"1-6"},"PeriodicalIF":2.9000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277077/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection Control and Hospital Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1017/ice.2025.90","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
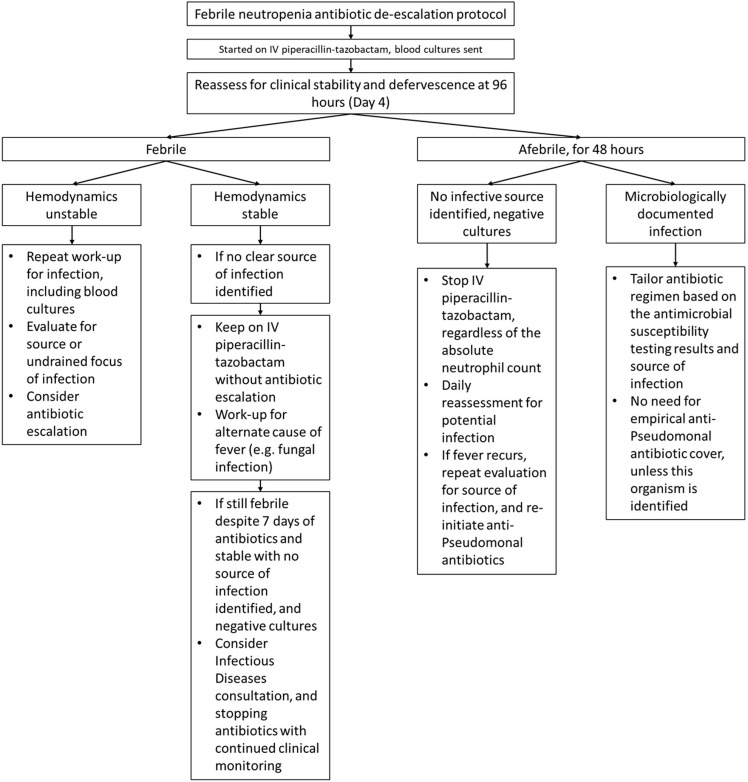
Background: Broad-spectrum antibiotic use in febrile neutropenia is often driven by concerns for severe and drug-resistant infections. In select patients who do not have an active infection and improve, their prolonged and unnecessary use contributes to antimicrobial resistance, drug toxicity, and increased healthcare costs. We describe the implementation of an antibiotic de-escalation protocol to reduce inappropriate antibiotic use in febrile neutropenia among hematology patients.
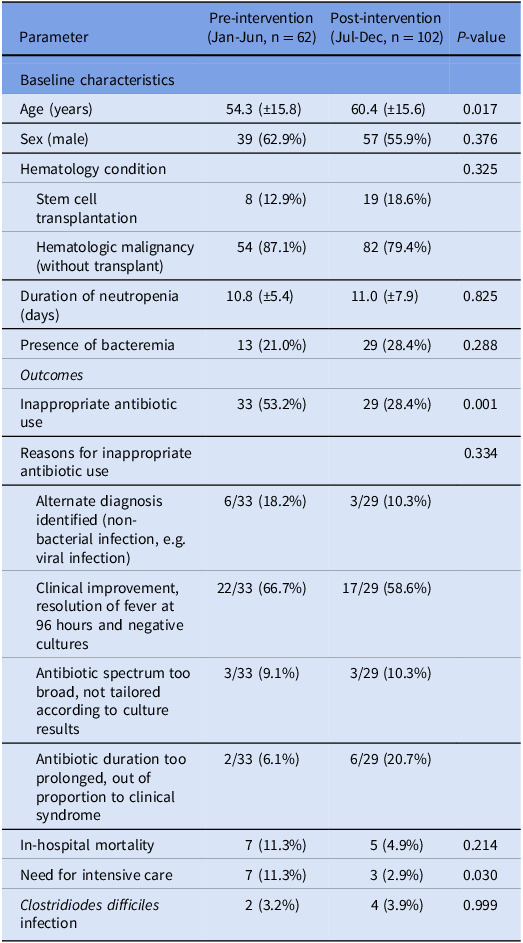
Methods: We conducted baseline analysis (January-June 2024) of antibiotic use in febrile neutropenia cases admitted under hematology. Interventions included the (i) development of an antibiotic de-escalation protocol to guide clinical management, (ii) a roadshow to educate and improve uptake of this protocol, and (iii) regular feedback via "report cards" for hematology teams. The primary outcome was the proportion of febrile neutropenia cases with inappropriate antibiotic use, with secondary measures including adverse outcomes (in-hospital mortality, Clostridioides difficile infection, need for intensive care).
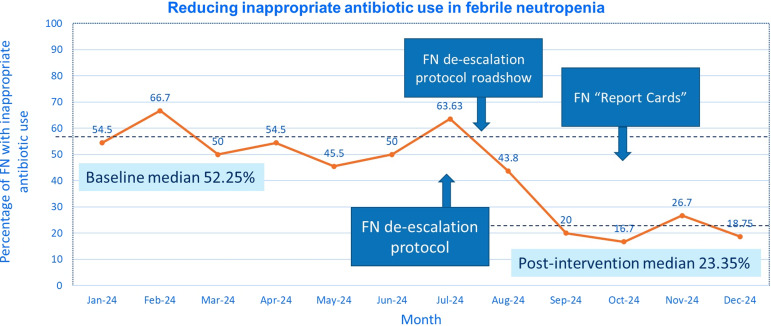
Results: Baseline data indicated inappropriate antibiotic use rates of 45.5-66.7% per month from January to June 2024, with 13-28 days of inappropriate therapy. The protocol was developed in July 2024, with a subsequent roadshow to promote its uptake. Regular feedback was provided in the form of "report cards" every 2-monthly thereafter. Post-intervention, inappropriate antibiotic use decreased to a median of 23.35% from July to December 2024, with no observed increase in adverse outcomes.
Conclusions: The implementation of a structured de-escalation protocol, combined with frequent education and feedback, effectively reduced inappropriate antibiotic use in febrile neutropenia without compromising patient safety.
期刊介绍:
Infection Control and Hospital Epidemiology provides original, peer-reviewed scientific articles for anyone involved with an infection control or epidemiology program in a hospital or healthcare facility. Written by infection control practitioners and epidemiologists and guided by an editorial board composed of the nation''s leaders in the field, ICHE provides a critical forum for this vital information.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


