Maxwell Sandberg, Claudia Marie-Costa, Rachel Vancavage, Emily Ye, Gavin Underwood, Rainer Rodriguez, Emily Roebuck, Sean Catley, Jorge Seoane, Arjun Choudhary, Stephen Tranchina, Ashok Hemal, Alejandro R Rodriguez
{"title":"Postoperative complications, emergency department utilisation, and readmission after radical cystectomy.","authors":"Maxwell Sandberg, Claudia Marie-Costa, Rachel Vancavage, Emily Ye, Gavin Underwood, Rainer Rodriguez, Emily Roebuck, Sean Catley, Jorge Seoane, Arjun Choudhary, Stephen Tranchina, Ashok Hemal, Alejandro R Rodriguez","doi":"10.5173/ceju.2024.0166","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>There is minimal research on the types of complications patients experience after radical cystectomy (RC). Moreover, the impact of these complications is not well qualified. The primary purpose of this study is to qualify complications after RC and quantify rates of emergency department (ED) utilisation and readmissions to the hospital. The secondary purpose is to associate risk factors for ED visits and hospital readmission.</p><p><strong>Material and methods: </strong>Patients were retrospectively analysed, who underwent RC for bladder cancer. ED visits within 90 days of discharge from RC and readmission at both 30 and 31-90 days of discharge were collected. Complications were graded using the Clavien-Dindo system and classified using the Memorial Sloan-Kettering Cancer Center complication system.</p><p><strong>Results: </strong>Three hundred and eighty-six patients were included. The in-house complication rate before discharge was 36%, and the 90-day complication rate after discharge was 54.8%. 33.7% of patients had ≥1 ED visit postoperatively, 18.7% were readmitted within 30 days, and 17.3% within 31-90 days of discharge. The primary reason for ED presentation, readmission at 30 and 31-90 days was infection. Cutaneous ureterostomy (CU) was associated with greater likelihood of presentation to the ED and readmission 31-90 days postoperatively (p <0.01). Overall survival (OS) was worse in patients who presented to the ED and/or were readmitted at both the 30- and 31-90-day marks (p <0.01).</p><p><strong>Conclusions: </strong>ED utilisation and readmission rates after RC are high. The most common complication is infection. Patients with a CU are at higher risk for healthcare utilisation. OS is worse in patients with an ED visit or readmission to the hospital, and these patients may require closer monitoring.</p>","PeriodicalId":9744,"journal":{"name":"Central European Journal of Urology","volume":"78 1","pages":"5-13"},"PeriodicalIF":1.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12073520/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Central European Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5173/ceju.2024.0166","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: There is minimal research on the types of complications patients experience after radical cystectomy (RC). Moreover, the impact of these complications is not well qualified. The primary purpose of this study is to qualify complications after RC and quantify rates of emergency department (ED) utilisation and readmissions to the hospital. The secondary purpose is to associate risk factors for ED visits and hospital readmission.
Material and methods: Patients were retrospectively analysed, who underwent RC for bladder cancer. ED visits within 90 days of discharge from RC and readmission at both 30 and 31-90 days of discharge were collected. Complications were graded using the Clavien-Dindo system and classified using the Memorial Sloan-Kettering Cancer Center complication system.
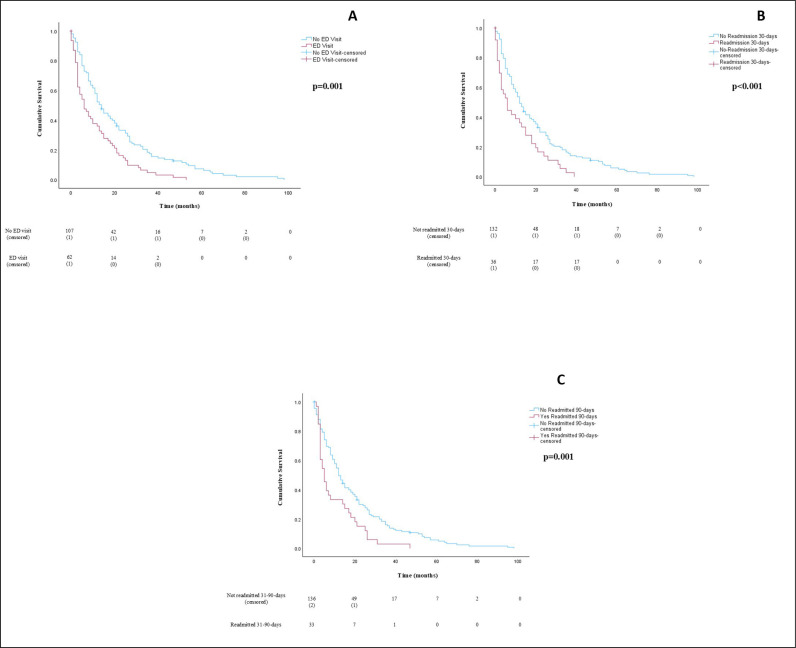
Results: Three hundred and eighty-six patients were included. The in-house complication rate before discharge was 36%, and the 90-day complication rate after discharge was 54.8%. 33.7% of patients had ≥1 ED visit postoperatively, 18.7% were readmitted within 30 days, and 17.3% within 31-90 days of discharge. The primary reason for ED presentation, readmission at 30 and 31-90 days was infection. Cutaneous ureterostomy (CU) was associated with greater likelihood of presentation to the ED and readmission 31-90 days postoperatively (p <0.01). Overall survival (OS) was worse in patients who presented to the ED and/or were readmitted at both the 30- and 31-90-day marks (p <0.01).
Conclusions: ED utilisation and readmission rates after RC are high. The most common complication is infection. Patients with a CU are at higher risk for healthcare utilisation. OS is worse in patients with an ED visit or readmission to the hospital, and these patients may require closer monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


