Risk stratification of node-positive early-stage cervical cancer treated with radical hysterectomy followed by chemoradiotherapy: a retrospective single-center study.
Shuang-Zheng Jia, Duan Yang, Xue-Jiao Yang, Rui Wang, Xi Yang, Man-Ni Huang, Ju-Sheng An
{"title":"Risk stratification of node-positive early-stage cervical cancer treated with radical hysterectomy followed by chemoradiotherapy: a retrospective single-center study.","authors":"Shuang-Zheng Jia, Duan Yang, Xue-Jiao Yang, Rui Wang, Xi Yang, Man-Ni Huang, Ju-Sheng An","doi":"10.1186/s13014-025-02655-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited data exist on the effectiveness of concurrent chemoradiotherapy (CRT) using intensity-modulated radiation therapy (IMRT) after radical surgery in patients with node-positive early-stage cervical cancer. This study aimed to identify prognostic factors and categorize patients into risk groups for personalized adjuvant therapy.</p><p><strong>Methods: </strong>The study included consecutive patients with pathologically confirmed node-positive cervical cancer who underwent radical hysterectomy and lymphadenectomy followed by CRT from January 2013 to October 2024 at our institute. Patients with parametrial invasion or positive resection margins were excluded. All patients received modern volumetric-modulated arc therapy with platinum-based concurrent chemotherapy. Data on clinicopathologic features, treatment details, and oncologic outcomes were collected. Univariate and multivariate Cox regression analyses were conducted to identify factors associated with disease-free survival (DFS) and overall survival (OS). Patients were further stratified into distinct risk categories for recurrence based on identified prognostic factors.</p><p><strong>Results: </strong>A total of 160 patients were included, with a median age of 44 years. The median number of lymph nodes retrieved was 33, and 11 patients presented with para-aortic lymph node metastasis (LNM). Over a median follow-up period of 39.7 months, 31 patients experienced disease progression, and 12 succumbed to the disease, yielding 3-year DFS and OS rates of 81.3% and 93.7%, respectively. Multivariate analysis identified non-squamous histotype (hazard ratio [HR]: 1.526, 95% confidence interval [CI]: 1.044-2.232, p = 0.029) and LNM ≥ 4 (HR: 1.521, 95% CI: 1.027-2.252, p = 0.036) as independent predictors of poorer DFS. Utilizing these prognostic factors for DFS, a risk stratification system was developed, categorizing patients into low-risk (no risk factors, n = 108) and high-intermediate risk (one or two risk factors, n = 52) groups. The high-intermediate-risk group exhibited significantly inferior DFS and OS compared to the low-risk group (3-year DFS: 67.4% versus 87.3%, HR: 1.697, 95% CI: 1.192-2.417, p = 0.002; 3-year OS: 82.5% versus 98.8%, HR: 3.577, 95% CI: 1.668-7.667, p < 0.001, respectively).</p><p><strong>Conclusions: </strong>Node-positive early-stage cervical cancer exhibits heterogeneous outcomes following radical hysterectomy and postoperative CRT. In patients with non-SCC histotype or ≥ 4 LNM, consolidation chemotherapy does not confer an additional survival benefit, indicating a need for innovative therapeutic strategies.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"73"},"PeriodicalIF":3.3000,"publicationDate":"2025-05-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076833/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02655-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Limited data exist on the effectiveness of concurrent chemoradiotherapy (CRT) using intensity-modulated radiation therapy (IMRT) after radical surgery in patients with node-positive early-stage cervical cancer. This study aimed to identify prognostic factors and categorize patients into risk groups for personalized adjuvant therapy.
Methods: The study included consecutive patients with pathologically confirmed node-positive cervical cancer who underwent radical hysterectomy and lymphadenectomy followed by CRT from January 2013 to October 2024 at our institute. Patients with parametrial invasion or positive resection margins were excluded. All patients received modern volumetric-modulated arc therapy with platinum-based concurrent chemotherapy. Data on clinicopathologic features, treatment details, and oncologic outcomes were collected. Univariate and multivariate Cox regression analyses were conducted to identify factors associated with disease-free survival (DFS) and overall survival (OS). Patients were further stratified into distinct risk categories for recurrence based on identified prognostic factors.
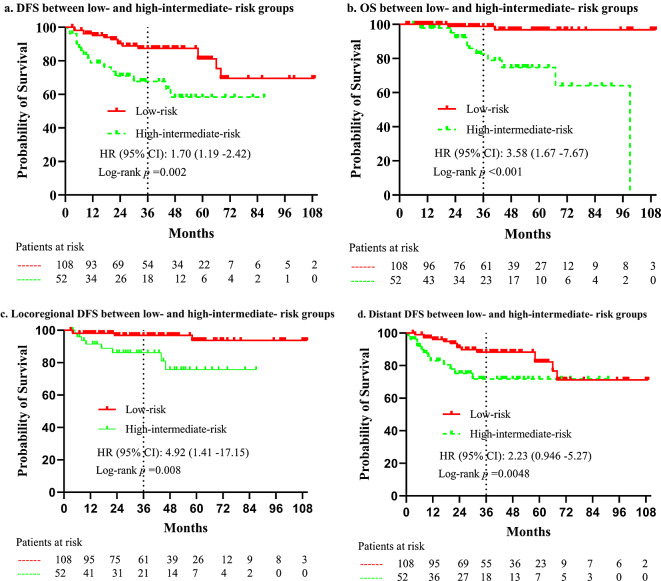
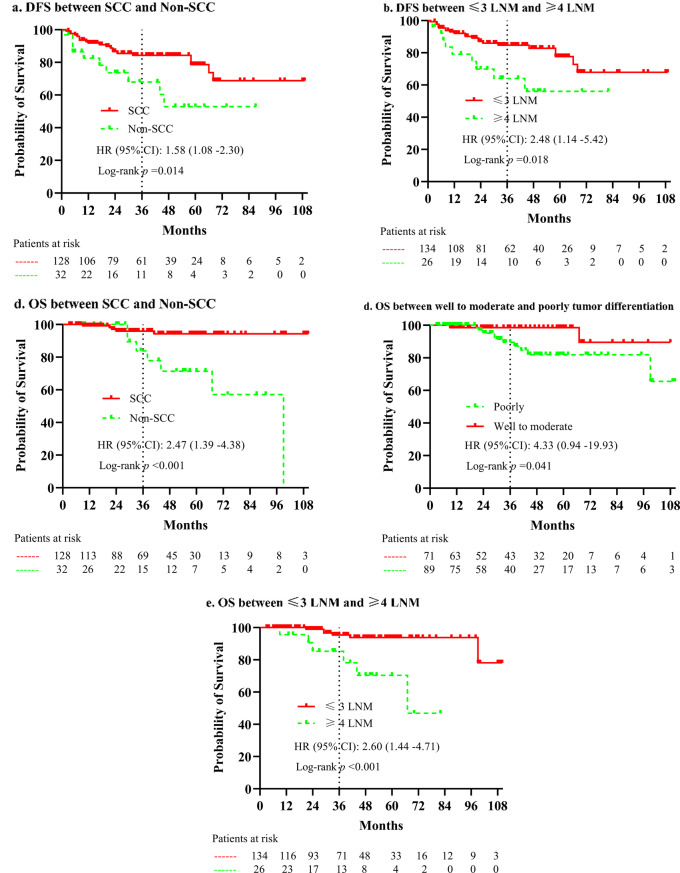
Results: A total of 160 patients were included, with a median age of 44 years. The median number of lymph nodes retrieved was 33, and 11 patients presented with para-aortic lymph node metastasis (LNM). Over a median follow-up period of 39.7 months, 31 patients experienced disease progression, and 12 succumbed to the disease, yielding 3-year DFS and OS rates of 81.3% and 93.7%, respectively. Multivariate analysis identified non-squamous histotype (hazard ratio [HR]: 1.526, 95% confidence interval [CI]: 1.044-2.232, p = 0.029) and LNM ≥ 4 (HR: 1.521, 95% CI: 1.027-2.252, p = 0.036) as independent predictors of poorer DFS. Utilizing these prognostic factors for DFS, a risk stratification system was developed, categorizing patients into low-risk (no risk factors, n = 108) and high-intermediate risk (one or two risk factors, n = 52) groups. The high-intermediate-risk group exhibited significantly inferior DFS and OS compared to the low-risk group (3-year DFS: 67.4% versus 87.3%, HR: 1.697, 95% CI: 1.192-2.417, p = 0.002; 3-year OS: 82.5% versus 98.8%, HR: 3.577, 95% CI: 1.668-7.667, p < 0.001, respectively).
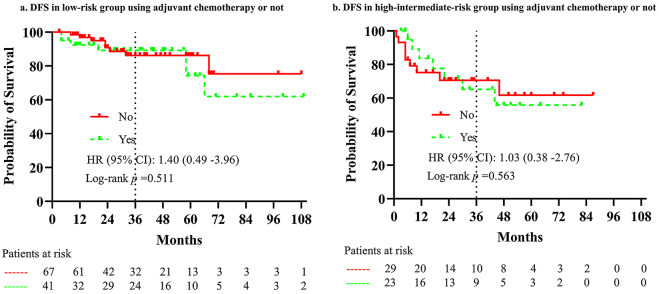
Conclusions: Node-positive early-stage cervical cancer exhibits heterogeneous outcomes following radical hysterectomy and postoperative CRT. In patients with non-SCC histotype or ≥ 4 LNM, consolidation chemotherapy does not confer an additional survival benefit, indicating a need for innovative therapeutic strategies.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


