The relation between delayed reperfusion treatment and reduced left ventricular ejection fraction in patients with ST-segment elevation myocardial infarction: a national prospective cohort study.
Bård Uleberg, Kaare Harald Bønaa, Kari Krizak Halle, Bjarne K Jacobsen, Beate Hauglann, Eva Stensland, Olav Helge Førde
{"title":"The relation between delayed reperfusion treatment and reduced left ventricular ejection fraction in patients with ST-segment elevation myocardial infarction: a national prospective cohort study.","authors":"Bård Uleberg, Kaare Harald Bønaa, Kari Krizak Halle, Bjarne K Jacobsen, Beate Hauglann, Eva Stensland, Olav Helge Førde","doi":"10.1093/ehjopen/oeaf034","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The aim of this nationwide study of patients with acute ST-segment elevation myocardial infarction (STEMI) was to investigate the relation between delayed reperfusion and mildly to moderately reduced and severely reduced left ventricular ejection fraction (LVEF).</p><p><strong>Methods and results: </strong>In this national population-based cohort study, log-binominal and modified Poisson regression models were applied to examine the associations between delayed reperfusion (i.e. fibrinolysis > 30 min or primary percutaneous coronary intervention > 120 min after first medical contact) and reduced LVEF, adjusted for reperfusion strategy, and patient characteristics. A total of 6567 Norwegian patients with STEMI registered in the Norwegian Registry of Myocardial Infarction during 2015-2018 were included in the analyses. Among them, 57% had normal LVEF (≥50%), 39% had mildly to moderately reduced LVEF (31-49%), and 4% had severely reduced LVEF (≤30%), measured during the acute admission. The adjusted relative risk of having a mildly to moderately reduced LVEF was 1.11 [95% confidence interval (CI) 1.04-1.18] for patients receiving delayed vs. timely reperfusion, and the adjusted relative risk of having severely reduced LVEF was 1.76 (95% CI 1.37-2.25) for patients receiving delayed vs. timely reperfusion. Reperfusion strategy, either primary percutaneous coronary intervention (pPCI) or a pharmacoinvasive strategy (PI), was not a significant determinant for reduced LVEF in any of the analyses.</p><p><strong>Conclusion: </strong>Delayed reperfusion treatment in STEMI increases the risk of mildly to moderately reduced LVEF, and the risk of severely reduced LVEF substantially, compared with timely reperfusion. The risk of reduced LVEF did not differ between patients treated with pPCI or PI.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 2","pages":"oeaf034"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001758/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
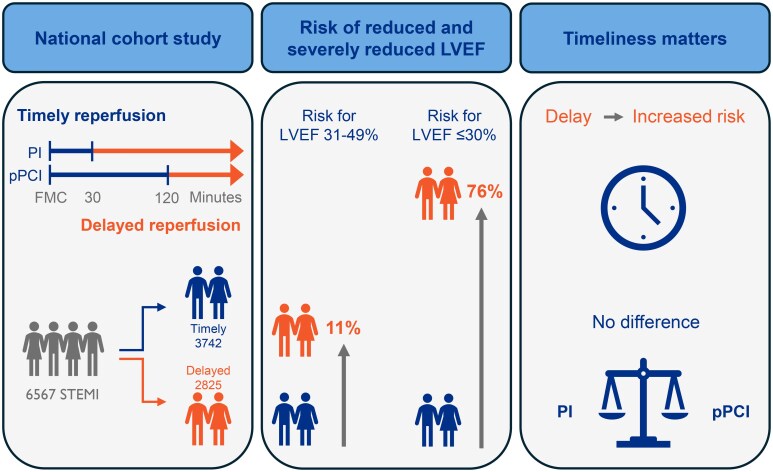
Aims: The aim of this nationwide study of patients with acute ST-segment elevation myocardial infarction (STEMI) was to investigate the relation between delayed reperfusion and mildly to moderately reduced and severely reduced left ventricular ejection fraction (LVEF).
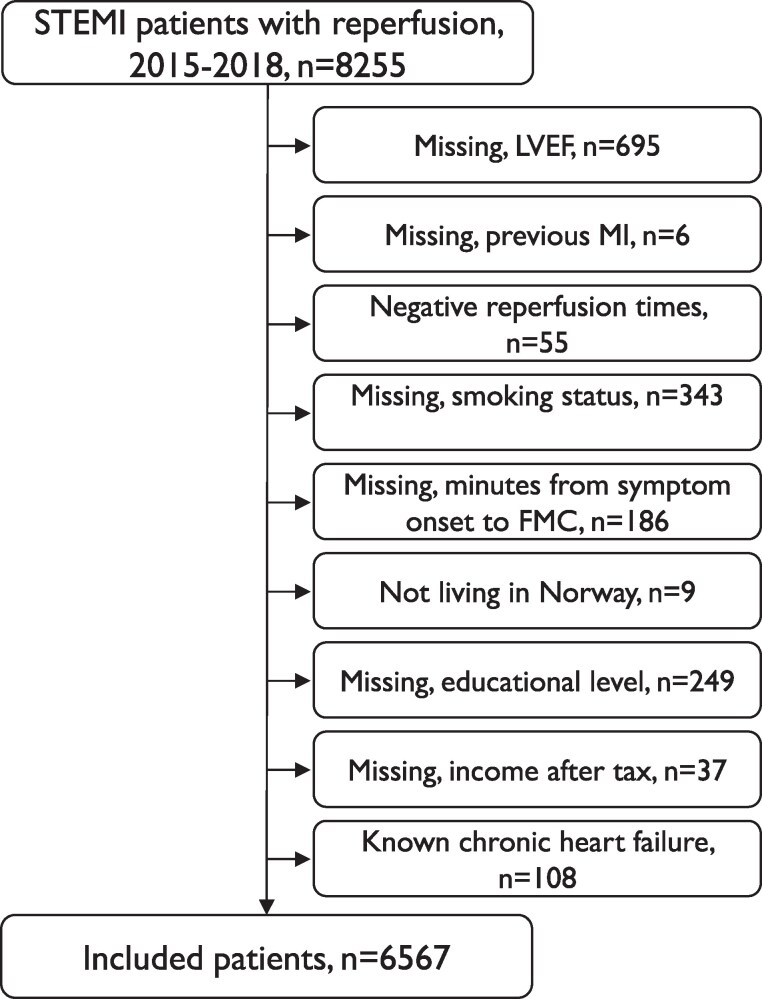
Methods and results: In this national population-based cohort study, log-binominal and modified Poisson regression models were applied to examine the associations between delayed reperfusion (i.e. fibrinolysis > 30 min or primary percutaneous coronary intervention > 120 min after first medical contact) and reduced LVEF, adjusted for reperfusion strategy, and patient characteristics. A total of 6567 Norwegian patients with STEMI registered in the Norwegian Registry of Myocardial Infarction during 2015-2018 were included in the analyses. Among them, 57% had normal LVEF (≥50%), 39% had mildly to moderately reduced LVEF (31-49%), and 4% had severely reduced LVEF (≤30%), measured during the acute admission. The adjusted relative risk of having a mildly to moderately reduced LVEF was 1.11 [95% confidence interval (CI) 1.04-1.18] for patients receiving delayed vs. timely reperfusion, and the adjusted relative risk of having severely reduced LVEF was 1.76 (95% CI 1.37-2.25) for patients receiving delayed vs. timely reperfusion. Reperfusion strategy, either primary percutaneous coronary intervention (pPCI) or a pharmacoinvasive strategy (PI), was not a significant determinant for reduced LVEF in any of the analyses.
Conclusion: Delayed reperfusion treatment in STEMI increases the risk of mildly to moderately reduced LVEF, and the risk of severely reduced LVEF substantially, compared with timely reperfusion. The risk of reduced LVEF did not differ between patients treated with pPCI or PI.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


