Brennan Donville, Heather Wolfe, Ken Tegtmeyer, Matthew Zackoff, Maria Frazier, Daniel Loeb, Andrew Lautz, Amanda O'Halloran, Maya Dewan
{"title":"Characteristics of Hot and Cold Debriefs for In-hospital Cardiac Arrest in the Pediatric Intensive Care Unit: A Mixed-methods Analysis.","authors":"Brennan Donville, Heather Wolfe, Ken Tegtmeyer, Matthew Zackoff, Maria Frazier, Daniel Loeb, Andrew Lautz, Amanda O'Halloran, Maya Dewan","doi":"10.1097/pq9.0000000000000812","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>This study examined a standardized event review approach, assessing hot and cold debriefs in pediatric in-hospital cardiac arrest (IHCA) to demonstrate their distinct but synergistic values.</p><p><strong>Methods: </strong>This retrospective mixed-methods analysis was conducted for 2 years in a large, single-center pediatric intensive care unit (PICU) at a quaternary care, free-standing children's hospital. Following the standardization of debriefing processes, both hot and cold debriefs were systematically performed after PICU IHCA events where chest compressions lasted longer than 1 minute, utilizing standardized debrief forms. Event-level data were collected for each IHCA, with the possibility of patients being represented multiple times.</p><p><strong>Results: </strong>There were 37 recorded PICU IHCAs during the study period from March 2020 to April 2022. Hot debriefs were performed in 84% (31/37) of events, and cold debriefs in 100% (37/37). Qualitative analysis of hot debriefs found that issues with communication and personnel (25%), cardiopulmonary resuscitation quality (25%), and medication preparation/administration (23.7%) were most cited. Analysis of cold debrief comments revealed that patient care (42.2%), environment and compliance (28.9%), and communication (20%) were the 3 most cited areas of potential improvement.</p><p><strong>Conclusions: </strong>Hot and cold debriefs following pediatric IHCA are both feasible and clinically valuable. The combined use of these debriefing tools provided more comprehensive insights, with each format uniquely contributing to identifying distinct areas for improvement. Additionally, our findings highlight the importance of a carefully crafted and standardized approach to debriefing that aligns with the intended outcomes.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"10 3","pages":"e812"},"PeriodicalIF":1.1000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12045529/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000812","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: This study examined a standardized event review approach, assessing hot and cold debriefs in pediatric in-hospital cardiac arrest (IHCA) to demonstrate their distinct but synergistic values.
Methods: This retrospective mixed-methods analysis was conducted for 2 years in a large, single-center pediatric intensive care unit (PICU) at a quaternary care, free-standing children's hospital. Following the standardization of debriefing processes, both hot and cold debriefs were systematically performed after PICU IHCA events where chest compressions lasted longer than 1 minute, utilizing standardized debrief forms. Event-level data were collected for each IHCA, with the possibility of patients being represented multiple times.
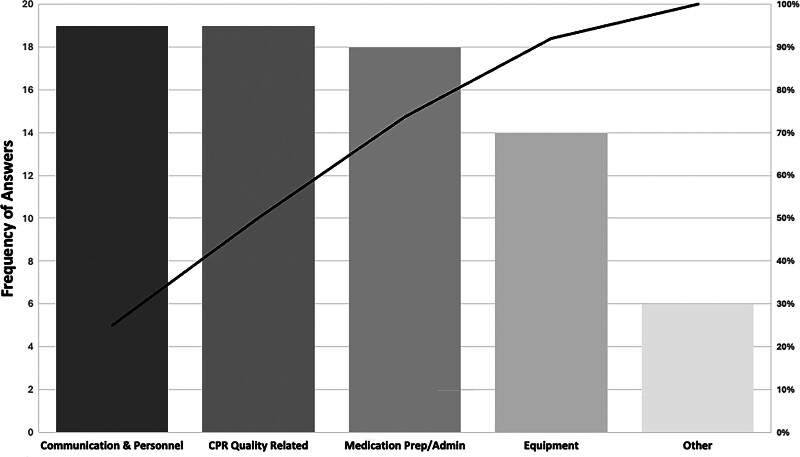
Results: There were 37 recorded PICU IHCAs during the study period from March 2020 to April 2022. Hot debriefs were performed in 84% (31/37) of events, and cold debriefs in 100% (37/37). Qualitative analysis of hot debriefs found that issues with communication and personnel (25%), cardiopulmonary resuscitation quality (25%), and medication preparation/administration (23.7%) were most cited. Analysis of cold debrief comments revealed that patient care (42.2%), environment and compliance (28.9%), and communication (20%) were the 3 most cited areas of potential improvement.
Conclusions: Hot and cold debriefs following pediatric IHCA are both feasible and clinically valuable. The combined use of these debriefing tools provided more comprehensive insights, with each format uniquely contributing to identifying distinct areas for improvement. Additionally, our findings highlight the importance of a carefully crafted and standardized approach to debriefing that aligns with the intended outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


