Reduced dose direct oral anticoagulants and time-in-therapeutic-range defined warfarin in new-onset atrial fibrillation: a report from the nationwide FinACAF study.
Alex Luojus, Mika Lehto, Olli Halminen, Ossi Lehtonen, Mikko Niemi, Konsta Teppo, Jaana Kuoppala, Jari Haukka, Jukka Putaala, Miika Linna, Pirjo Mustonen, Aapo Aro, Juha Hartikainen, Gregory Yoke Hong Lip, Kari Eino Juhani Airaksinen
{"title":"Reduced dose direct oral anticoagulants and time-in-therapeutic-range defined warfarin in new-onset atrial fibrillation: a report from the nationwide FinACAF study.","authors":"Alex Luojus, Mika Lehto, Olli Halminen, Ossi Lehtonen, Mikko Niemi, Konsta Teppo, Jaana Kuoppala, Jari Haukka, Jukka Putaala, Miika Linna, Pirjo Mustonen, Aapo Aro, Juha Hartikainen, Gregory Yoke Hong Lip, Kari Eino Juhani Airaksinen","doi":"10.1093/ehjopen/oeaf046","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Direct oral anticoagulants (DOACs) at reduced dosage regimens are the first choice of ischaemic stroke (IS) prevention for patients with atrial fibrillation (AF) and elevated bleeding risk or renal insufficiency. We compared the outcomes of reduced dose DOACs and warfarin.</p><p><strong>Methods and results: </strong>We included all new-onset patients with AF in Finland from 2011 to 2018. Adjusted hazard ratios (HRs) for IS, intracranial haemorrhage (ICH), bleeding, and mortality were calculated for dabigatran (<i>n</i> = 2 672), rivaroxaban (<i>n</i> = 1 866), apixaban (<i>n</i> = 3 936), and warfarin (<i>n</i> = 43 548). Patients on warfarin were grouped into quartiles by their individual time-in-therapeutic range (TTR), with the second best TTR quartile as a reference group for comparisons. Risk of IS was highest in the low TTR quartiles of warfarin, lowest in the best TTR quartile (0.65 95% confidence interval, 0.51-0.83), and did not differ for dabigatran, rivaroxaban, and apixaban compared with the second best TTR quartile. Risk of ICH was highest in low TTR quartiles of warfarin (HRs 7.20, 5.48-9.46 and 1.91, 1.44-2.55), and was not different in patients on dabigatran, rivaroxaban, and apixaban. Risk of all-cause death and bleeding were lowest in the two best TTR quartiles, and highest in the poorest TTR group. Mortality was higher for dabigatran, rivaroxaban, and apixaban, compared with the second best TTR quartile of warfarin.</p><p><strong>Conclusion: </strong>DOACs with reduced doses are efficient and safe stroke prevention therapy in high-risk patients with AF when compared with warfarin therapy of sufficient TTR. In this comparison, warfarin therapy of excellent TTR-quality was associated with the lowest risk of bleeding and mortality.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf046"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12066950/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
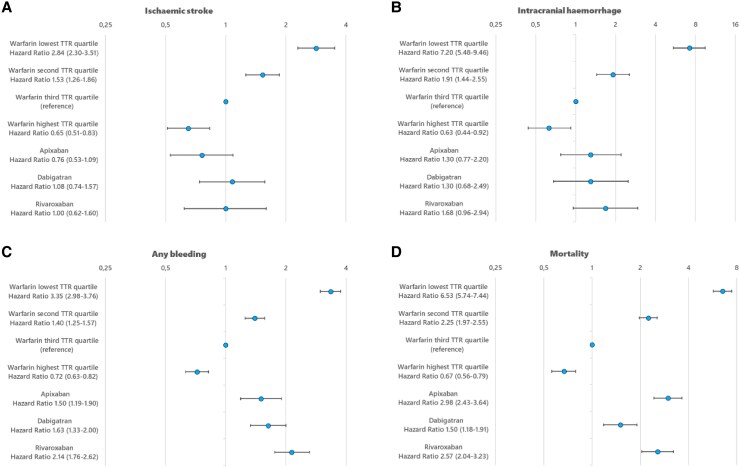
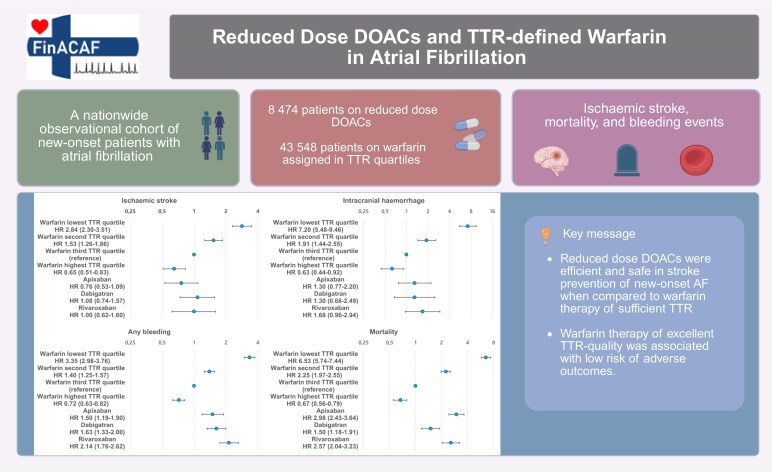
Aims: Direct oral anticoagulants (DOACs) at reduced dosage regimens are the first choice of ischaemic stroke (IS) prevention for patients with atrial fibrillation (AF) and elevated bleeding risk or renal insufficiency. We compared the outcomes of reduced dose DOACs and warfarin.
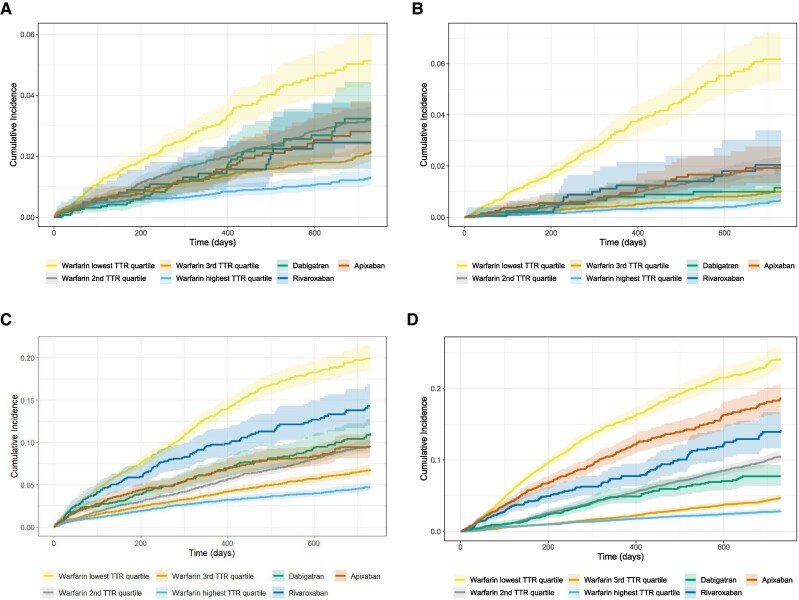
Methods and results: We included all new-onset patients with AF in Finland from 2011 to 2018. Adjusted hazard ratios (HRs) for IS, intracranial haemorrhage (ICH), bleeding, and mortality were calculated for dabigatran (n = 2 672), rivaroxaban (n = 1 866), apixaban (n = 3 936), and warfarin (n = 43 548). Patients on warfarin were grouped into quartiles by their individual time-in-therapeutic range (TTR), with the second best TTR quartile as a reference group for comparisons. Risk of IS was highest in the low TTR quartiles of warfarin, lowest in the best TTR quartile (0.65 95% confidence interval, 0.51-0.83), and did not differ for dabigatran, rivaroxaban, and apixaban compared with the second best TTR quartile. Risk of ICH was highest in low TTR quartiles of warfarin (HRs 7.20, 5.48-9.46 and 1.91, 1.44-2.55), and was not different in patients on dabigatran, rivaroxaban, and apixaban. Risk of all-cause death and bleeding were lowest in the two best TTR quartiles, and highest in the poorest TTR group. Mortality was higher for dabigatran, rivaroxaban, and apixaban, compared with the second best TTR quartile of warfarin.
Conclusion: DOACs with reduced doses are efficient and safe stroke prevention therapy in high-risk patients with AF when compared with warfarin therapy of sufficient TTR. In this comparison, warfarin therapy of excellent TTR-quality was associated with the lowest risk of bleeding and mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


