Tristan M F Buck, Jason A H Steman, Jari Dahmen, Quinten G H Rikken, Inger N Sierevelt, Sjoerd A S Stufkens, Gino M M J Kerkhoffs
{"title":"Nonoperative Treatment for Osteochondral Lesions of the Talus Provides Clinical Improvement in the Minority of the Patients at Short-term Follow-up.","authors":"Tristan M F Buck, Jason A H Steman, Jari Dahmen, Quinten G H Rikken, Inger N Sierevelt, Sjoerd A S Stufkens, Gino M M J Kerkhoffs","doi":"10.1177/10711007251330881","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Often, the preferred initial treatment for osteochondral lesions of the talus (OLTs) is nonoperative for at least 6 months before considering more invasive surgical strategies. The primary aim of this study was to evaluate the clinical effectiveness of nonoperative management for OLTs on prospective clinical outcomes over a 1-year period. Secondary aims included assessing the radiologic outcomes, the rate of conversion to surgery, and the influence of baseline factors on return to a higher level of activity.</p><p><strong>Methods: </strong>Patients who underwent nonoperative management for primary OLTs were prospectively included. Clinical outcome measures were assessed at baseline, 6 months, and 12 months. The primary outcome of this prospective cohort study is the change in the numeric rating scale (NRS) for pain score during walking between baseline and 12 months. Secondary outcomes included changes in NRS during rest, NRS during running, NRS during stair climbing, Foot and Ankle Outcome Scale (FAOS) subscales, changes in lesion volume and surface area, and conversion to surgery rate.</p><p><strong>Results: </strong>A total of 40 patients (42 ankles) mean age 31.6 years with a primary symptomatic OLT were included. The primary outcome, NRS during walking, significantly improved between 0 and 12 months (4.8 to 3.3; <i>P</i> = .0003). However, the mean decrease did not exceed the minimal clinically important difference (MCID), with only 38% of the patients exceeding the MCID at 12-month follow-up. NRS scores during running and stair climbing showed improvements from baseline to 6 months (<i>P</i> = .0004 and <i>P</i> = .002) and from baseline to 12 months (<i>P</i> = .0001 and <i>P</i> = .0002). None of these average NRS change scores at 12-month follow-up exceeded the MCID. FAOS sports and quality of life subscales improved significantly from baseline to 6 months (<i>P</i> = .003 and <i>P</i> = .011) and remained stable from 6 to 12 months. The FAOS pain subscale showed significant improvement only after 12 months. Lesion sizes remained stable throughout the one-year period.</p><p><strong>Conclusion: </strong>Nonoperative treatment resulted in statistically significant improvements in pain during walking after 1 year, with clinically relevant improvement observed in 38% of patients. These findings suggest that nonoperative treatment held the potential for meaningfully improving symptoms in the minority of our patients, with no appreciable change in OLTT size. We think it should be considered as a preferred approach for the first line of treatment.</p>","PeriodicalId":94011,"journal":{"name":"Foot & ankle international","volume":" ","pages":"699-706"},"PeriodicalIF":2.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12227802/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & ankle international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/10711007251330881","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Often, the preferred initial treatment for osteochondral lesions of the talus (OLTs) is nonoperative for at least 6 months before considering more invasive surgical strategies. The primary aim of this study was to evaluate the clinical effectiveness of nonoperative management for OLTs on prospective clinical outcomes over a 1-year period. Secondary aims included assessing the radiologic outcomes, the rate of conversion to surgery, and the influence of baseline factors on return to a higher level of activity.
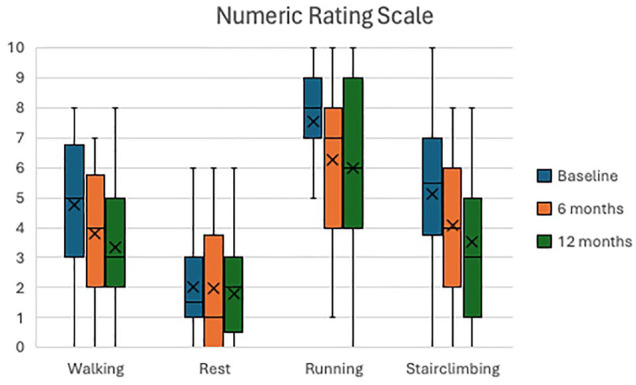
Methods: Patients who underwent nonoperative management for primary OLTs were prospectively included. Clinical outcome measures were assessed at baseline, 6 months, and 12 months. The primary outcome of this prospective cohort study is the change in the numeric rating scale (NRS) for pain score during walking between baseline and 12 months. Secondary outcomes included changes in NRS during rest, NRS during running, NRS during stair climbing, Foot and Ankle Outcome Scale (FAOS) subscales, changes in lesion volume and surface area, and conversion to surgery rate.
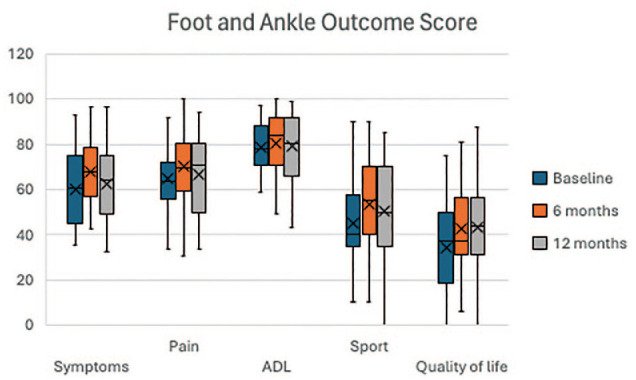
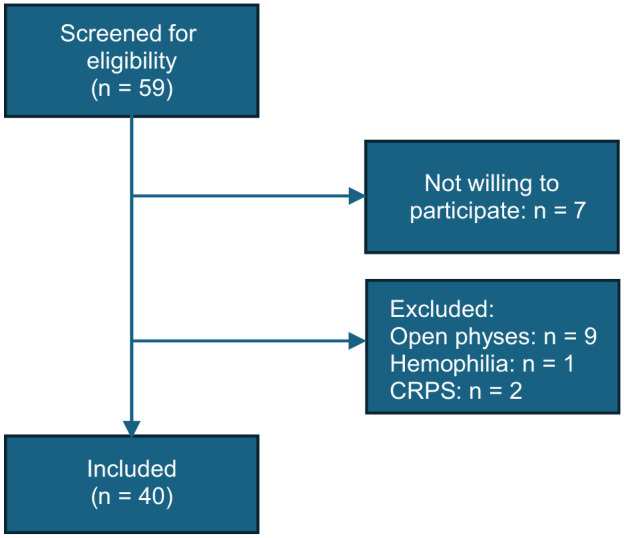
Results: A total of 40 patients (42 ankles) mean age 31.6 years with a primary symptomatic OLT were included. The primary outcome, NRS during walking, significantly improved between 0 and 12 months (4.8 to 3.3; P = .0003). However, the mean decrease did not exceed the minimal clinically important difference (MCID), with only 38% of the patients exceeding the MCID at 12-month follow-up. NRS scores during running and stair climbing showed improvements from baseline to 6 months (P = .0004 and P = .002) and from baseline to 12 months (P = .0001 and P = .0002). None of these average NRS change scores at 12-month follow-up exceeded the MCID. FAOS sports and quality of life subscales improved significantly from baseline to 6 months (P = .003 and P = .011) and remained stable from 6 to 12 months. The FAOS pain subscale showed significant improvement only after 12 months. Lesion sizes remained stable throughout the one-year period.
Conclusion: Nonoperative treatment resulted in statistically significant improvements in pain during walking after 1 year, with clinically relevant improvement observed in 38% of patients. These findings suggest that nonoperative treatment held the potential for meaningfully improving symptoms in the minority of our patients, with no appreciable change in OLTT size. We think it should be considered as a preferred approach for the first line of treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


