Qualitative analysis of patient and key informant interviews to inform integration of HIV pre-exposure prophylaxis services into gynecology care in Alabama.
Madeline C Pratt, Hannah Goymer, Kaylee Burgan, Lynn T Matthews, Bernadette Johnson, Desiree Phillips, Mirjam-Colette Kempf, Michael J Mugavero, Audra Williams, Latesha E Elopre
{"title":"Qualitative analysis of patient and key informant interviews to inform integration of HIV pre-exposure prophylaxis services into gynecology care in Alabama.","authors":"Madeline C Pratt, Hannah Goymer, Kaylee Burgan, Lynn T Matthews, Bernadette Johnson, Desiree Phillips, Mirjam-Colette Kempf, Michael J Mugavero, Audra Williams, Latesha E Elopre","doi":"10.1177/17455057251331714","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>HIV pre-exposure prophylaxis (PrEP) use is low among Southern, Black cis-gender women (CGW). Gynecology clinics are well-positioned to integrate PrEP services as a component of sexual and reproductive healthcare for CGW.</p><p><strong>Objectives: </strong>Identify key determinants to PrEP implementation into routine gynecologic care.</p><p><strong>Design: </strong>Qualitative, in-depth interviews (IDIs).</p><p><strong>Methods: </strong>We conducted IDIs with key informants (i.e., physicians, nurses, medical assistants) and focus group discussions (FGDs) with patients accessing care in a gynecology clinic serving under- and uninsured women in Alabama. IDIs explored individual-, setting-, and process-level factors that may impact PrEP care implementation in a clinic serving approximately 3000 women yearly, 64% of whom are Black women.</p><p><strong>Results: </strong>Ten key informants participated in individual IDIs (median age 33.5, range 24-58 years, 80% female); 20 women participated in either 1 of 4 FGDs (<i>n</i> = 8) or an individual IDI (<i>n</i> = 12); median age 32, range 19-44. The following themes emerged: (1) patient- and provider-level stigmas related to sexuality, sexually transmitted infections (STIs), and HIV limit discussions about sexual health and HIV prevention. (2) Providers report limited knowledge about prescribing and monitoring PrEP, which is reflected in patient's observations that providers do not routinely initiate discussions about HIV prevention or PrEP. (3) Providers utilize a more risk-based approach to PrEP counseling; patients expect non-targeted, comprehensive sexual health information. (4) Structural and social barriers will be challenges to implementing PrEP in routine gynecological care. (5) Patients and providers support a clinic-wide approach to integration of PrEP into gynecology clinics.</p><p><strong>Conclusion: </strong>Discussions around sexual health and STIs are limited in routine gynecologic care, but patients expect comprehensive counseling from knowledgeable providers. Additional provider training may increase comfort discussing and providing PrEP. These findings will inform development of implementation strategies to integrate PrEP care into gynecologic services.</p>","PeriodicalId":75327,"journal":{"name":"Women's health (London, England)","volume":"21 ","pages":"17455057251331714"},"PeriodicalIF":2.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12062644/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Women's health (London, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17455057251331714","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/8 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: HIV pre-exposure prophylaxis (PrEP) use is low among Southern, Black cis-gender women (CGW). Gynecology clinics are well-positioned to integrate PrEP services as a component of sexual and reproductive healthcare for CGW.
Objectives: Identify key determinants to PrEP implementation into routine gynecologic care.
Design: Qualitative, in-depth interviews (IDIs).
Methods: We conducted IDIs with key informants (i.e., physicians, nurses, medical assistants) and focus group discussions (FGDs) with patients accessing care in a gynecology clinic serving under- and uninsured women in Alabama. IDIs explored individual-, setting-, and process-level factors that may impact PrEP care implementation in a clinic serving approximately 3000 women yearly, 64% of whom are Black women.
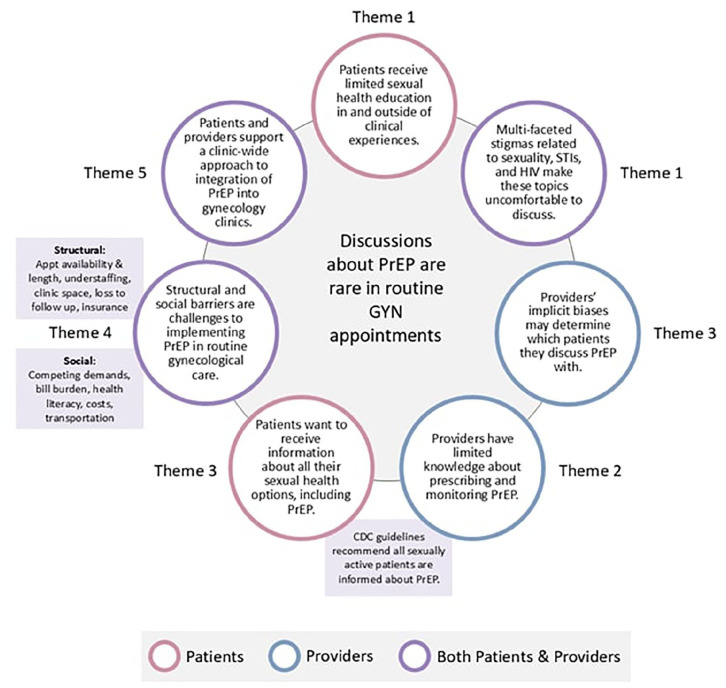
Results: Ten key informants participated in individual IDIs (median age 33.5, range 24-58 years, 80% female); 20 women participated in either 1 of 4 FGDs (n = 8) or an individual IDI (n = 12); median age 32, range 19-44. The following themes emerged: (1) patient- and provider-level stigmas related to sexuality, sexually transmitted infections (STIs), and HIV limit discussions about sexual health and HIV prevention. (2) Providers report limited knowledge about prescribing and monitoring PrEP, which is reflected in patient's observations that providers do not routinely initiate discussions about HIV prevention or PrEP. (3) Providers utilize a more risk-based approach to PrEP counseling; patients expect non-targeted, comprehensive sexual health information. (4) Structural and social barriers will be challenges to implementing PrEP in routine gynecological care. (5) Patients and providers support a clinic-wide approach to integration of PrEP into gynecology clinics.
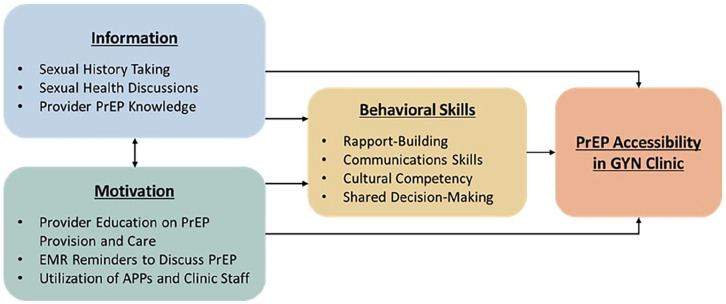
Conclusion: Discussions around sexual health and STIs are limited in routine gynecologic care, but patients expect comprehensive counseling from knowledgeable providers. Additional provider training may increase comfort discussing and providing PrEP. These findings will inform development of implementation strategies to integrate PrEP care into gynecologic services.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


