Tamaryn Fox, Leor Needleman, Krishna L Bharani, Frederick Mihm, Justin P Annes, Julia J Chang
{"title":"Functional Suppression of a Prolactinoma by a Dopamine-Secreting Paraganglioma.","authors":"Tamaryn Fox, Leor Needleman, Krishna L Bharani, Frederick Mihm, Justin P Annes, Julia J Chang","doi":"10.1210/jcemcr/luaf080","DOIUrl":null,"url":null,"abstract":"<p><p>Prolactin-secreting pituitary adenomas are typically treated with dopamine agonists to inhibit prolactin secretion and reduce tumor size. Dopamine-secreting paragangliomas are rare neuroendocrine tumors of sympathetic and parasympathetic paraganglia and often do not provoke symptoms of catecholamine excess. Although overlapping genetic drivers have been described for paragangliomas and pituitary adenomas, biochemical crosstalk between coexisting tumors is underexplored. We describe the case of a 52-year-old male individual who presented with cerebrospinal fluid (CSF) rhinorrhea and was found to have an invasive, 4.2-cm pituitary mass with modestly elevated prolactin (130.9 ng/mL [130.9 µg/L], reference range [RR] 2-18 ng/mL [2-18 µg/L]). Additional imaging discovered a mediastinal mass suspicious for a thoracic paraganglioma. Biochemical screening demonstrated marked elevation of plasma and urinary dopamine. Following paraganglioma resection, dopamine levels normalized, but prolactin rose significantly (877.8 ng/mL [877.8 µg/L]), suggesting an endogenous dopamine agonist-like effect from the paraganglioma to suppress pituitary prolactin hypersecretion. Pituitary pathology was notable for a PIT1 (pituitary transcription factor-1)-lineage pituitary adenoma with absent immunohistochemical staining for prolactin. Genetic testing found a previously unreported germline <i>SDHC</i> variant of uncertain significance. In this case, we report a novel biologic signaling mechanism between 2 rare primary endocrine tumors and highlight challenges in their diagnosis and management.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"3 6","pages":"luaf080"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12011523/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luaf080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
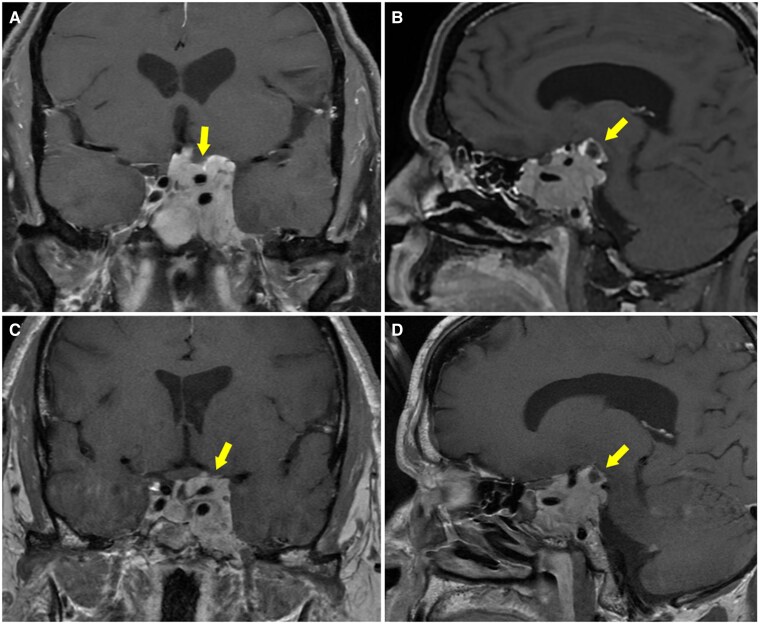
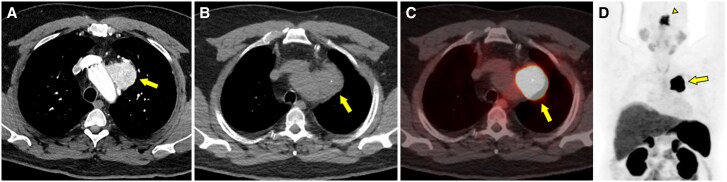
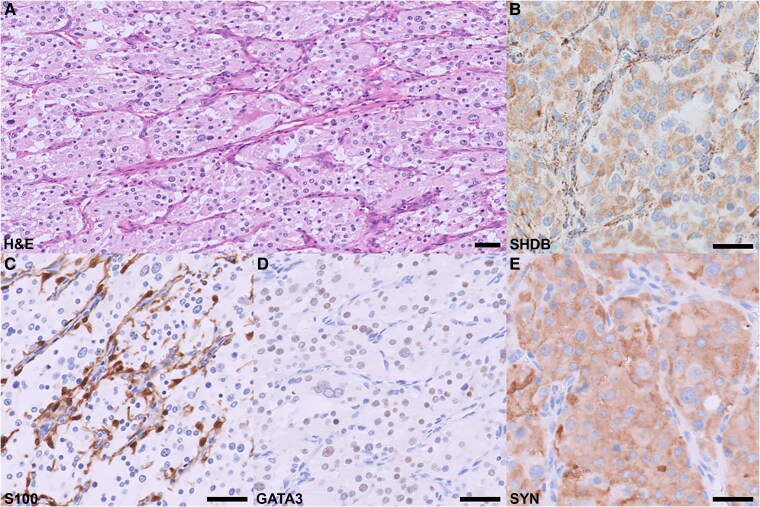
Prolactin-secreting pituitary adenomas are typically treated with dopamine agonists to inhibit prolactin secretion and reduce tumor size. Dopamine-secreting paragangliomas are rare neuroendocrine tumors of sympathetic and parasympathetic paraganglia and often do not provoke symptoms of catecholamine excess. Although overlapping genetic drivers have been described for paragangliomas and pituitary adenomas, biochemical crosstalk between coexisting tumors is underexplored. We describe the case of a 52-year-old male individual who presented with cerebrospinal fluid (CSF) rhinorrhea and was found to have an invasive, 4.2-cm pituitary mass with modestly elevated prolactin (130.9 ng/mL [130.9 µg/L], reference range [RR] 2-18 ng/mL [2-18 µg/L]). Additional imaging discovered a mediastinal mass suspicious for a thoracic paraganglioma. Biochemical screening demonstrated marked elevation of plasma and urinary dopamine. Following paraganglioma resection, dopamine levels normalized, but prolactin rose significantly (877.8 ng/mL [877.8 µg/L]), suggesting an endogenous dopamine agonist-like effect from the paraganglioma to suppress pituitary prolactin hypersecretion. Pituitary pathology was notable for a PIT1 (pituitary transcription factor-1)-lineage pituitary adenoma with absent immunohistochemical staining for prolactin. Genetic testing found a previously unreported germline SDHC variant of uncertain significance. In this case, we report a novel biologic signaling mechanism between 2 rare primary endocrine tumors and highlight challenges in their diagnosis and management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


