Rachel Hatcliffe, Anne Ciriello, Elizabeth Murphy Waibel, Cindy Colson, Ashley White, Jennifer Fritzeen, Sarah Isbey
{"title":"Pediatric Emergency Department Burn Discharge and Clinic Readiness: A Quality Improvement Project.","authors":"Rachel Hatcliffe, Anne Ciriello, Elizabeth Murphy Waibel, Cindy Colson, Ashley White, Jennifer Fritzeen, Sarah Isbey","doi":"10.1097/pq9.0000000000000806","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The shift to outpatient care for pediatric burn injuries has placed a greater responsibility on caregivers for wound care and follow-up planning. Nonadherence to burn care and follow-up appointments can lead to negative emotional and physical health outcomes. Both parental education and pain control with dressing changes are important factors for adherence to outpatient care. This single-center quality improvement project aimed to improve pediatric burn patients discharged from the emergency department with the correct instruction packet and the percentage of qualifying patients prescribed oxycodone for premedication for their initial clinic appointment.</p><p><strong>Methods: </strong>A multidisciplinary team retrospectively examined barriers using a fishbone diagram, developed a key driver diagram, and designed interventions, including updated custom instructions, printed discharge pamphlets, electronic medical record changes, enhanced e-prescribing access, linked International Classification of Diseases, Tenth Revision codes, targeted provider feedback, and education sessions. We tracked monthly data using statistical process control charts.</p><p><strong>Results: </strong>At baseline, 46% of patients received the correct discharge packet; following interventions, we observed a centerline shift to 78% with sustained improvement. Seventy percent of qualifying patients received an oxycodone prescription for premedication before clinic follow-up at baseline, and we saw a sustained baseline shift to 93% after interventions.</p><p><strong>Conclusions: </strong>Following multiple targeted interventions, there was a sustained improvement in the use of a custom burn discharge instruction packet and oxycodone prescriptions. Future research should examine the impact of discharge instructions and oxycodone prescriptions on the timeliness of outpatient appointment scheduling and pain scores.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"10 3","pages":"e806"},"PeriodicalIF":1.1000,"publicationDate":"2025-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12002377/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000806","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The shift to outpatient care for pediatric burn injuries has placed a greater responsibility on caregivers for wound care and follow-up planning. Nonadherence to burn care and follow-up appointments can lead to negative emotional and physical health outcomes. Both parental education and pain control with dressing changes are important factors for adherence to outpatient care. This single-center quality improvement project aimed to improve pediatric burn patients discharged from the emergency department with the correct instruction packet and the percentage of qualifying patients prescribed oxycodone for premedication for their initial clinic appointment.
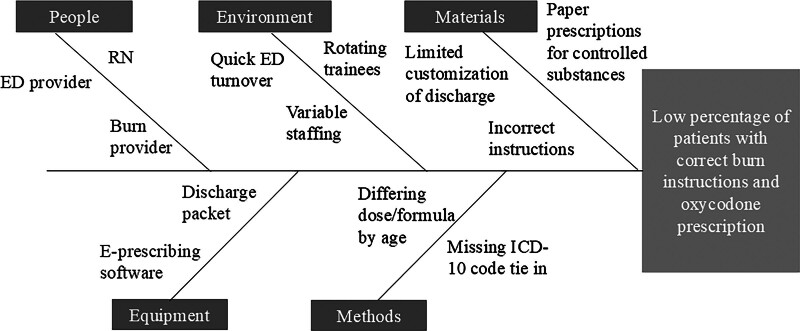
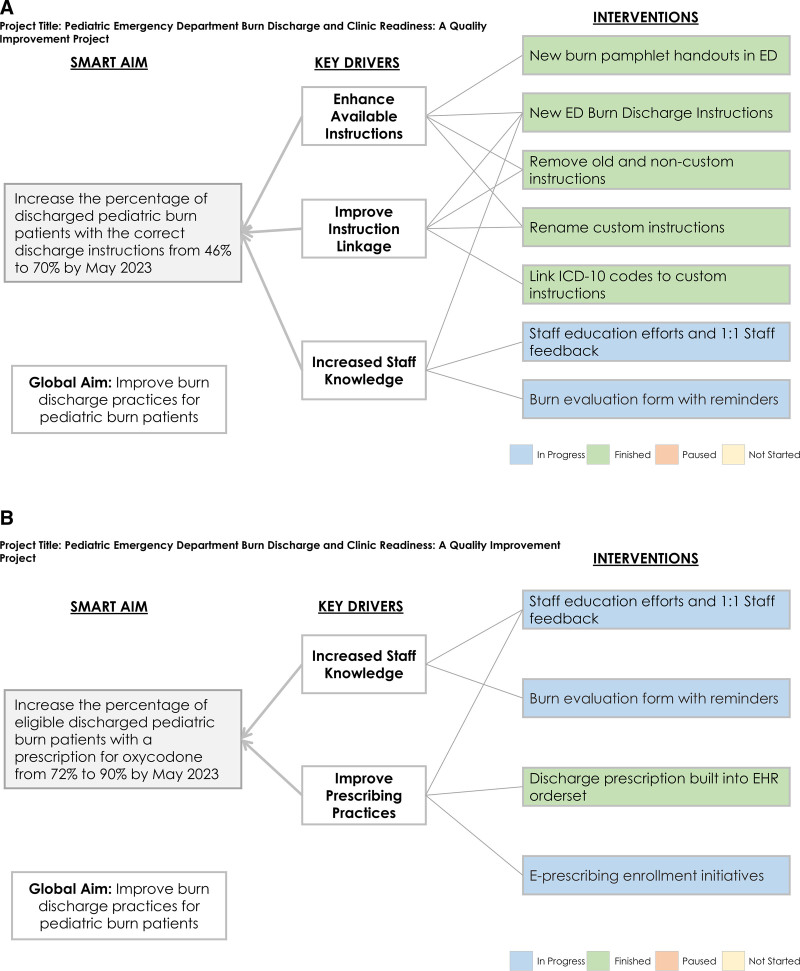
Methods: A multidisciplinary team retrospectively examined barriers using a fishbone diagram, developed a key driver diagram, and designed interventions, including updated custom instructions, printed discharge pamphlets, electronic medical record changes, enhanced e-prescribing access, linked International Classification of Diseases, Tenth Revision codes, targeted provider feedback, and education sessions. We tracked monthly data using statistical process control charts.
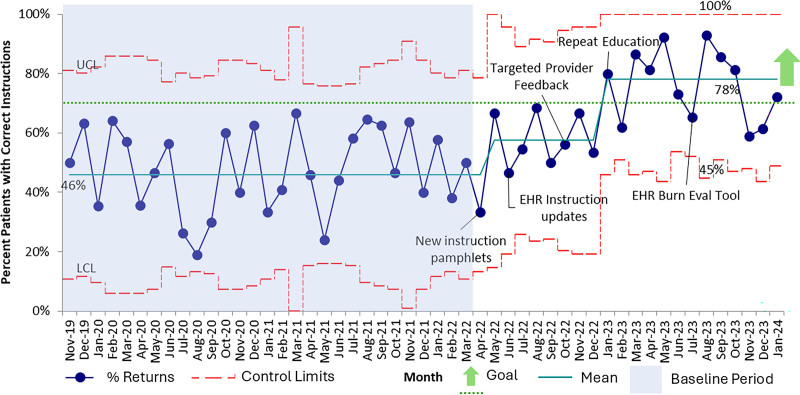
Results: At baseline, 46% of patients received the correct discharge packet; following interventions, we observed a centerline shift to 78% with sustained improvement. Seventy percent of qualifying patients received an oxycodone prescription for premedication before clinic follow-up at baseline, and we saw a sustained baseline shift to 93% after interventions.
Conclusions: Following multiple targeted interventions, there was a sustained improvement in the use of a custom burn discharge instruction packet and oxycodone prescriptions. Future research should examine the impact of discharge instructions and oxycodone prescriptions on the timeliness of outpatient appointment scheduling and pain scores.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


