Humphrey Gm Walker, Alexander S Richardson, Arne Diehl, Brooke Riley, Eldho Paul, Aidan Burrell
{"title":"Early fluid balance and mortality following extracorporeal cardiopulmonary resuscitation: a high volume, single center study.","authors":"Humphrey Gm Walker, Alexander S Richardson, Arne Diehl, Brooke Riley, Eldho Paul, Aidan Burrell","doi":"10.1186/s13049-025-01381-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For patients supported with venoarterial extracorporeal membrane oxygenation (VA-ECMO), a positive cumulative fluid balance at day three has been associated with increased mortality. However, there is limited evidence examining this association in patients requiring extracorporeal cardiopulmonary resuscitation (ECPR). The aims of this study were to (1) to describe contemporary fluid practice in patients requiring ECPR and (2) assess the relationship between early cumulative fluid balance and 28-day mortality.</p><p><strong>Methods: </strong>This was a retrospective, single centre, observational study using data collected from the EXCEL registry and the hospital electronic medical record. All patients undergoing ECPR from January 2017 until December 2022 were identified using a prospectively collected database. Patients aged < 18 years old or had extra-corporeal support ceased prior to arrival to the intensive care unit were excluded. Fluid data was collected for days 1,2,3 and 7; and cumulative balances reported for day 3 and day 7.</p><p><strong>Results: </strong>104 patients were identified, of which 100 were included. The mean age was 48.9 (SD 14.1) years, 72 (72%) were male. 54 (54%) were out-of-hospital cardiac arrests. Median low flow time was 43 (IQR 39-76) minutes. 51 (51%) had died by day 28. After adjusting for location of cardiac arrest, return of spontaneous circulation and duration of ECMO, a 1 L increase in cumulative fluid balance to the end of day 3 was not independently associated with 28-day mortality (adjusted OR 1.09 [95% CI 0.97-1.22]), however by day 7 this was independently associated with an 11% increased risk of 28-day mortality (adjusted OR 1.11 [95% CI 1.001-1.23]).</p><p><strong>Conclusion: </strong>A one litre increase in CFB at the end of day 3 was not associated with 28-day mortality; but a one litre increase in CFB by the end of day 7 was associated with an 11% increase in the odds of day 28 mortality. The impact of restrictive fluid management strategies in those requiring ECPR should be assessed in prospective trials.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"66"},"PeriodicalIF":3.1000,"publicationDate":"2025-04-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12016082/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01381-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
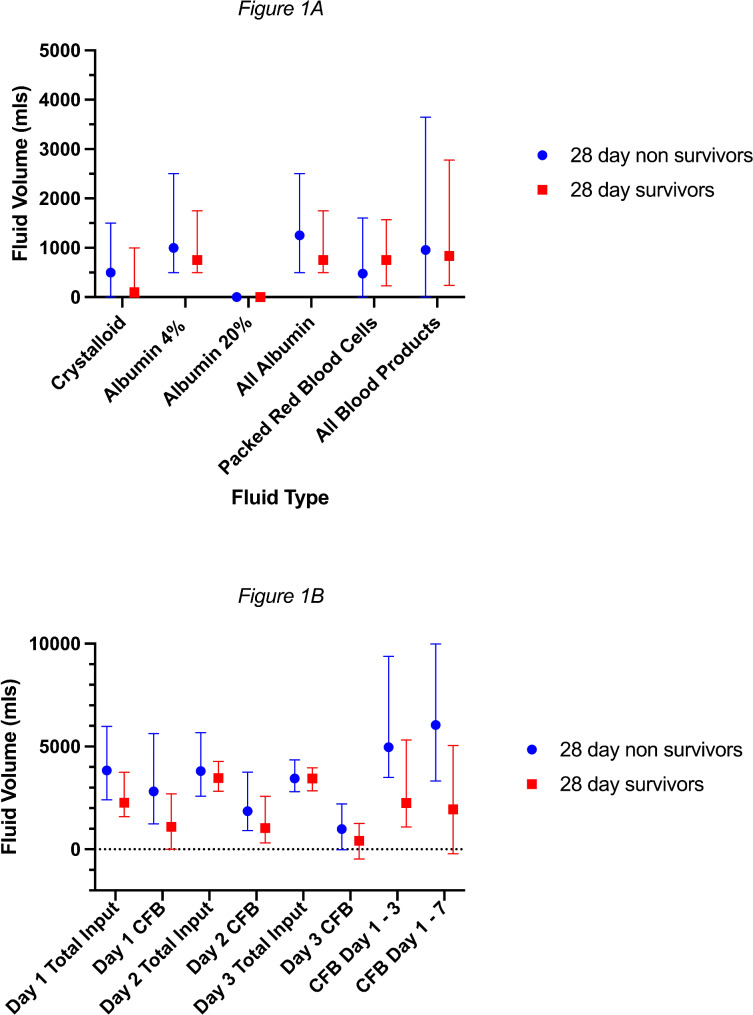
Background: For patients supported with venoarterial extracorporeal membrane oxygenation (VA-ECMO), a positive cumulative fluid balance at day three has been associated with increased mortality. However, there is limited evidence examining this association in patients requiring extracorporeal cardiopulmonary resuscitation (ECPR). The aims of this study were to (1) to describe contemporary fluid practice in patients requiring ECPR and (2) assess the relationship between early cumulative fluid balance and 28-day mortality.
Methods: This was a retrospective, single centre, observational study using data collected from the EXCEL registry and the hospital electronic medical record. All patients undergoing ECPR from January 2017 until December 2022 were identified using a prospectively collected database. Patients aged < 18 years old or had extra-corporeal support ceased prior to arrival to the intensive care unit were excluded. Fluid data was collected for days 1,2,3 and 7; and cumulative balances reported for day 3 and day 7.
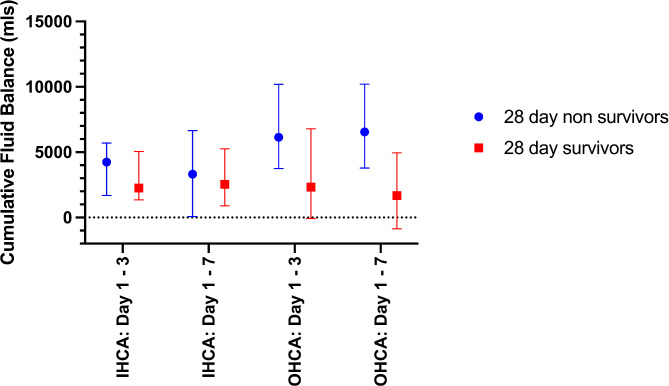
Results: 104 patients were identified, of which 100 were included. The mean age was 48.9 (SD 14.1) years, 72 (72%) were male. 54 (54%) were out-of-hospital cardiac arrests. Median low flow time was 43 (IQR 39-76) minutes. 51 (51%) had died by day 28. After adjusting for location of cardiac arrest, return of spontaneous circulation and duration of ECMO, a 1 L increase in cumulative fluid balance to the end of day 3 was not independently associated with 28-day mortality (adjusted OR 1.09 [95% CI 0.97-1.22]), however by day 7 this was independently associated with an 11% increased risk of 28-day mortality (adjusted OR 1.11 [95% CI 1.001-1.23]).
Conclusion: A one litre increase in CFB at the end of day 3 was not associated with 28-day mortality; but a one litre increase in CFB by the end of day 7 was associated with an 11% increase in the odds of day 28 mortality. The impact of restrictive fluid management strategies in those requiring ECPR should be assessed in prospective trials.
背景:对于静脉动脉体外膜氧合(VA-ECMO)支持的患者,第3天的累积体液平衡阳性与死亡率增加有关。然而,在需要体外心肺复苏(ECPR)的患者中,这种关联的证据有限。本研究的目的是:(1)描述需要ECPR的患者的当代液体实践;(2)评估早期累积液体平衡与28天死亡率之间的关系。方法:这是一项回顾性、单中心、观察性研究,数据收集自EXCEL注册表和医院电子病历。使用前瞻性收集的数据库确定2017年1月至2022年12月期间接受ECPR的所有患者。结果:确定104例患者,其中纳入100例。平均年龄48.9岁(SD 14.1),男性72例(72%)。54例(54%)院外心脏骤停。中位低流时间为43分钟(IQR 39-76)。51例(51%)在第28天死亡。在调整心脏骤停位置、自发循环恢复和ECMO持续时间后,到第3天结束时,累积液体平衡增加1 L与28天死亡率没有独立关联(调整后的OR为1.09 [95% CI 0.97-1.22]),但到第7天,这与28天死亡率风险增加11%独立相关(调整后的OR为1.11 [95% CI 1.001-1.23])。结论:第3天结束时CFB增加1升与28天死亡率无关;但在第7天结束时,CFB每增加1升,第28天的死亡率就会增加11%。限制性液体管理策略对需要ECPR的患者的影响应在前瞻性试验中进行评估。
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


