Jennifer Elston Lafata, Katharine A Rendle, Jocelyn V Wainwright, Mary E Cooley, Anil Vachani, Christine Neslund-Dudas, Michelle R Odelberg, Liana Alcaro, Claire Staresinic, Gwen L Alexander, Rebecca B Carlson, Marilyn M Schapira
{"title":"Characterizing the Design of and Emerging Evidence for Health Care Organization-Based Lung Cancer Screening Interventions: A Systematic Review.","authors":"Jennifer Elston Lafata, Katharine A Rendle, Jocelyn V Wainwright, Mary E Cooley, Anil Vachani, Christine Neslund-Dudas, Michelle R Odelberg, Liana Alcaro, Claire Staresinic, Gwen L Alexander, Rebecca B Carlson, Marilyn M Schapira","doi":"10.1177/23814683251328375","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background.</b> Implementing a lung cancer screening (LCS) program with low-dose computed tomography (LDCT) is complex, requiring health care organizations to consider several steps along the screening continuum from eligibility assessment to recommended follow-up testing adherence. The evidence to support LDCT screening implementation remains unclear. <b>Purpose.</b> To summarize interventions facilitating LCS initiation, adoption, or improvement within health care organizations. <b>Data Sources.</b> Librarian-assisted literature reviews identified published studies between January 1, 2011, and December 31, 2023, using CINAHL, Cochrane Library, Embase, Ovid Medline, PsycINFO, and Scopus. <b>Study Selection.</b> Published interventions focusing on any step in the LCS process before lung cancer diagnosis, including risk/eligibility assessment, shared decision making (SDM), and annual screening or diagnostic testing. <b>Data Abstraction.</b> We used a title/abstract review process, full-text review, and risk-of-bias assessments. We characterized studies by design, unit of observation, participant sociodemographic characteristics, primary outcome, and step in the LCS process. DistillerSR and Covidence were used for data management. <b>Data Synthesis.</b> We identified 64 study-eligible published articles, including 19 randomized and 45 nonrandomized studies. SDM interventions were most frequently studied (<i>n</i> = 20) followed by initial LCS uptake (<i>n</i> = 12). Most studies (<i>n</i> = 33) evaluated educational interventions, typically in one-on-one settings. Studies assessed at either low or moderate/some risk of bias reported statistically significant findings in the domains of improved knowledge (<i>n</i> = 7) and other aspects of decision making (<i>n</i> = 8), such as perceived risk or decisional conflict. Findings regarding LCS uptake were more variable. <b>Limitations.</b> The review includes only English-language studies published prior to 2024. The risk of bias was high among 5 of the randomized clinical trials and serious among 27 of the quasi-experimental design studies. <b>Conclusions.</b> LCS intervention strategies have focused on SDM and initial LCS uptake, leaving gaps in knowledge about how to support risk and eligibility assessment, adherence to annual screening, or diagnostic testing. Expanding interventions beyond those that are education focused and with single-level targets would expand the LDCT screening implementation evidence base.</p><p><strong>Highlights: </strong>Most lung cancer screening (LCS) interventions evaluated to date have been educational in nature and focused primarily on shared decision making or the initial uptake of screening, with some interventions demonstrating statistically significant improvements in patient knowledge and initial LCS order/uptake.A critical gap in knowledge remains regarding how to effectively support LCS eligibility assessment as well as adherence to annual screening and appropriate diagnostic testing.Findings underscore the need for the field to expand beyond education-focused interventions and incorporate multilevel targets when designing interventions to support high-quality LCS in practice.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"10 1","pages":"23814683251328375"},"PeriodicalIF":1.7000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12035285/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683251328375","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
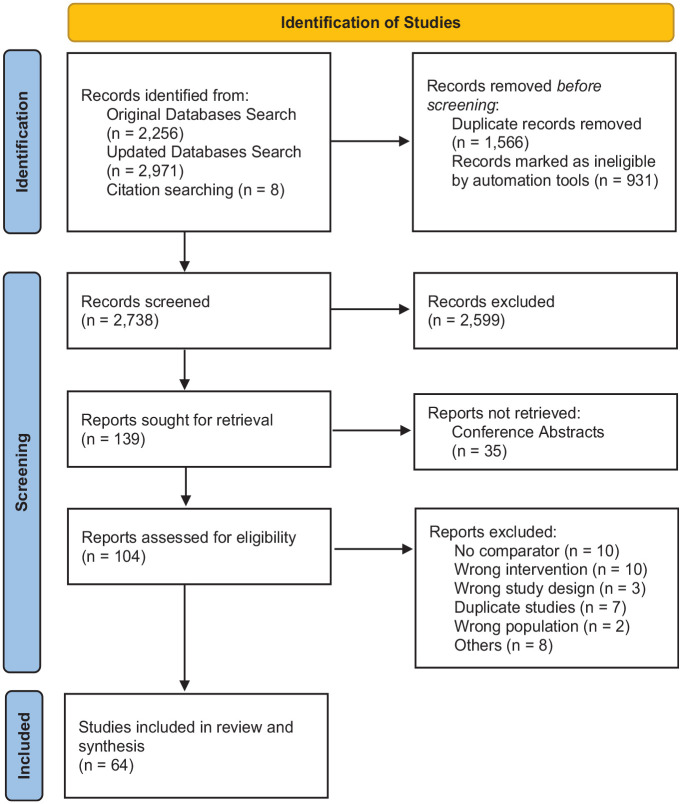
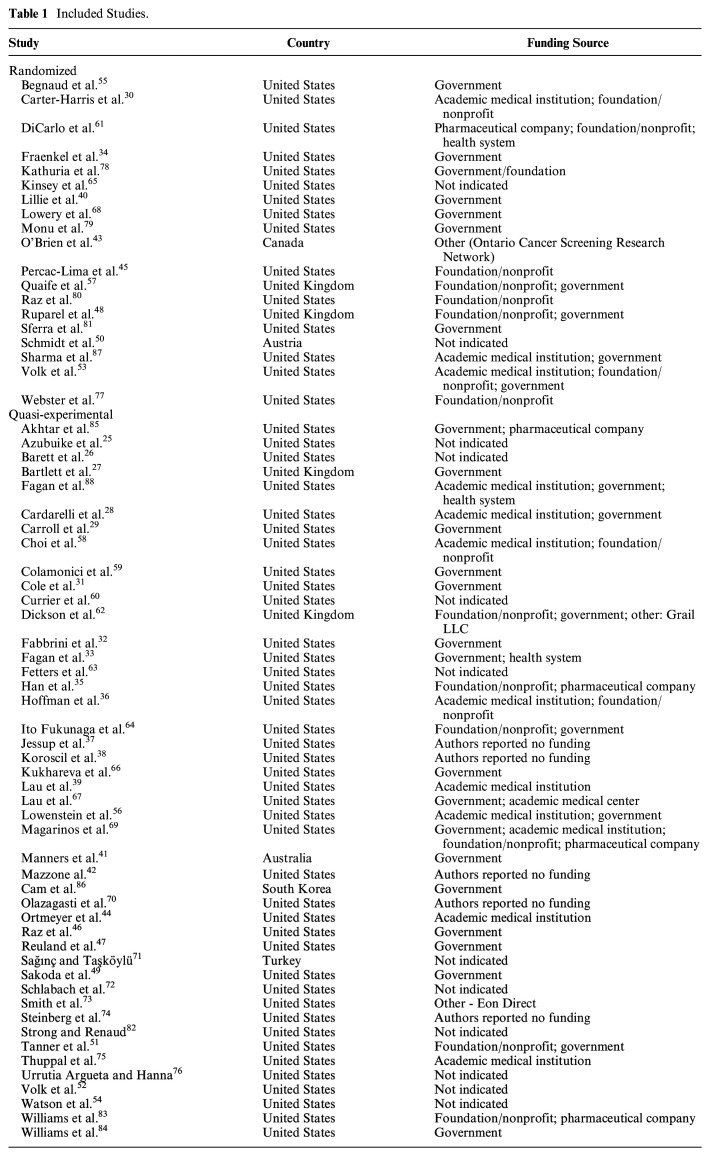
Background. Implementing a lung cancer screening (LCS) program with low-dose computed tomography (LDCT) is complex, requiring health care organizations to consider several steps along the screening continuum from eligibility assessment to recommended follow-up testing adherence. The evidence to support LDCT screening implementation remains unclear. Purpose. To summarize interventions facilitating LCS initiation, adoption, or improvement within health care organizations. Data Sources. Librarian-assisted literature reviews identified published studies between January 1, 2011, and December 31, 2023, using CINAHL, Cochrane Library, Embase, Ovid Medline, PsycINFO, and Scopus. Study Selection. Published interventions focusing on any step in the LCS process before lung cancer diagnosis, including risk/eligibility assessment, shared decision making (SDM), and annual screening or diagnostic testing. Data Abstraction. We used a title/abstract review process, full-text review, and risk-of-bias assessments. We characterized studies by design, unit of observation, participant sociodemographic characteristics, primary outcome, and step in the LCS process. DistillerSR and Covidence were used for data management. Data Synthesis. We identified 64 study-eligible published articles, including 19 randomized and 45 nonrandomized studies. SDM interventions were most frequently studied (n = 20) followed by initial LCS uptake (n = 12). Most studies (n = 33) evaluated educational interventions, typically in one-on-one settings. Studies assessed at either low or moderate/some risk of bias reported statistically significant findings in the domains of improved knowledge (n = 7) and other aspects of decision making (n = 8), such as perceived risk or decisional conflict. Findings regarding LCS uptake were more variable. Limitations. The review includes only English-language studies published prior to 2024. The risk of bias was high among 5 of the randomized clinical trials and serious among 27 of the quasi-experimental design studies. Conclusions. LCS intervention strategies have focused on SDM and initial LCS uptake, leaving gaps in knowledge about how to support risk and eligibility assessment, adherence to annual screening, or diagnostic testing. Expanding interventions beyond those that are education focused and with single-level targets would expand the LDCT screening implementation evidence base.
Highlights: Most lung cancer screening (LCS) interventions evaluated to date have been educational in nature and focused primarily on shared decision making or the initial uptake of screening, with some interventions demonstrating statistically significant improvements in patient knowledge and initial LCS order/uptake.A critical gap in knowledge remains regarding how to effectively support LCS eligibility assessment as well as adherence to annual screening and appropriate diagnostic testing.Findings underscore the need for the field to expand beyond education-focused interventions and incorporate multilevel targets when designing interventions to support high-quality LCS in practice.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


