Milton Chin, Mona Haj, Sarah L Versnel, Henriette H W de Gier, Eppo B Wolvius
{"title":"Obstructive Sleep Apnea Following Secondary Velopharyngeal Insufficiency in Children with Non-Syndromic Cleft Palate: A Systematic Review.","authors":"Milton Chin, Mona Haj, Sarah L Versnel, Henriette H W de Gier, Eppo B Wolvius","doi":"10.3390/cmtr18010006","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Systematic review.</p><p><strong>Objective: </strong>Obstructive sleep apnea (OSA) is a possible complication following secondary velopharyngeal insufficiency surgery in patients with repaired cleft palate. Various surgical techniques are used to treat secondary velopharyngeal insufficiency after cleft palate repair, but the optimal procedure remains debatable. This review provides an overview of the incidence of airway obstructive outcomes related to different surgical modalities.</p><p><strong>Methods: </strong>A systematic search was performed on the 1st of February following the PRISMA guidelines and registered on PROSPERO (CRD42022299715). The following databases were reviewed: Medline, EMBASE, Web of Science, Google Scholar, and the Cochrane Library databases. Studies that included data on the occurrence of OSA following velopharyngeal surgery in children with a repaired non-syndromic cleft palate were included. Non-English articles and studies that included syndromic cleft palate patients were excluded.</p><p><strong>Results: </strong>Twenty-eight articles met the inclusion criteria. The surgical procedures are classified into three groups: pharyngeal flap procedure (PF), sphincter pharyngoplasty (SP), and palatal muscle repositioning (PMR). Incidence of post-operative OSA and symptoms of OSA were lowest after PMR compared to SP and PF (3%; 34%; 29%, respectively). Pharyngeal flap procedures resulted in the best speech outcomes.</p><p><strong>Conclusions: </strong>PMR results in fewer postoperative complications in terms of OSA and achieves a satisfactory reduction in hypernasal speech. PF procedure carries a higher risk of developing OSA postoperatively but seems to be superior in the reduction in hypernasality.</p>","PeriodicalId":46447,"journal":{"name":"Craniomaxillofacial Trauma & Reconstruction","volume":"18 1","pages":"6"},"PeriodicalIF":0.4000,"publicationDate":"2025-01-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11995821/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Craniomaxillofacial Trauma & Reconstruction","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/cmtr18010006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: Systematic review.
Objective: Obstructive sleep apnea (OSA) is a possible complication following secondary velopharyngeal insufficiency surgery in patients with repaired cleft palate. Various surgical techniques are used to treat secondary velopharyngeal insufficiency after cleft palate repair, but the optimal procedure remains debatable. This review provides an overview of the incidence of airway obstructive outcomes related to different surgical modalities.
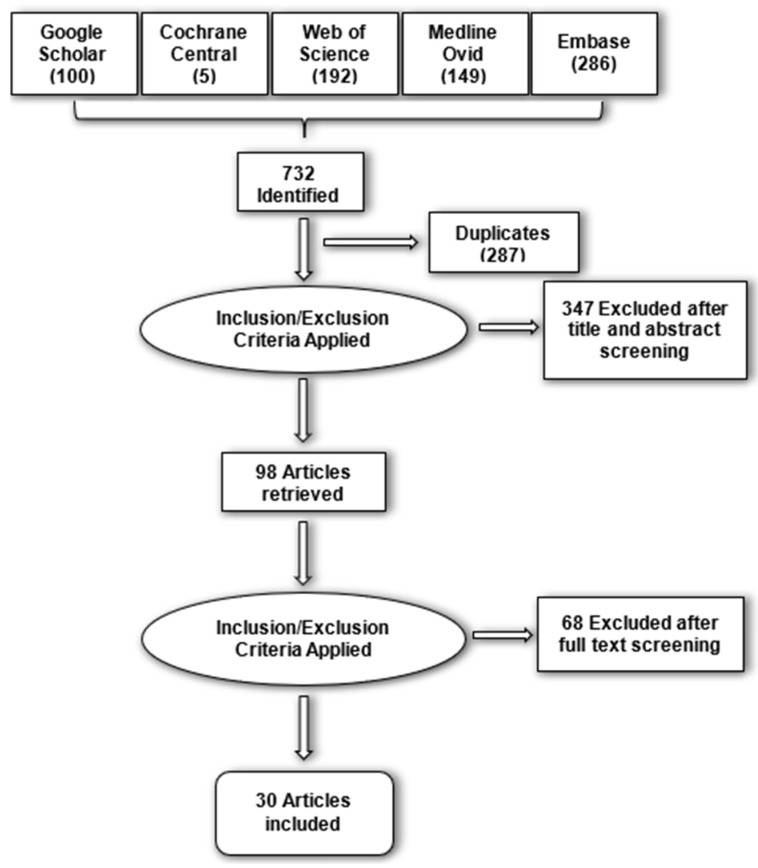
Methods: A systematic search was performed on the 1st of February following the PRISMA guidelines and registered on PROSPERO (CRD42022299715). The following databases were reviewed: Medline, EMBASE, Web of Science, Google Scholar, and the Cochrane Library databases. Studies that included data on the occurrence of OSA following velopharyngeal surgery in children with a repaired non-syndromic cleft palate were included. Non-English articles and studies that included syndromic cleft palate patients were excluded.
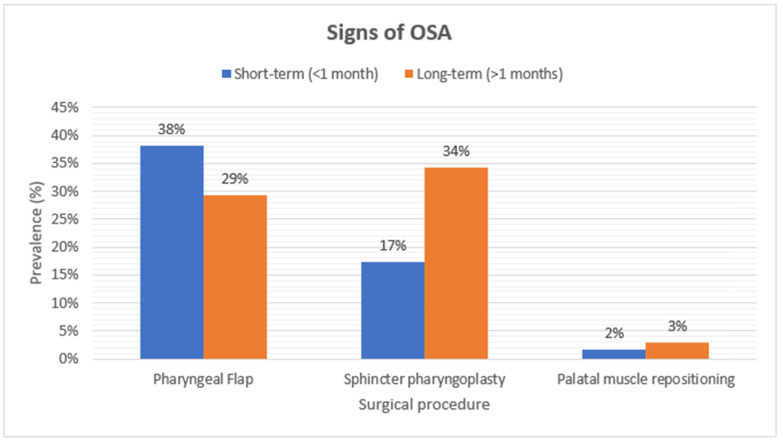
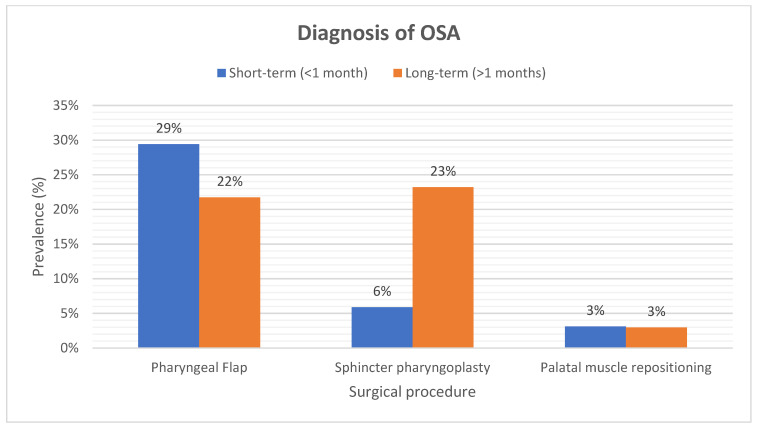
Results: Twenty-eight articles met the inclusion criteria. The surgical procedures are classified into three groups: pharyngeal flap procedure (PF), sphincter pharyngoplasty (SP), and palatal muscle repositioning (PMR). Incidence of post-operative OSA and symptoms of OSA were lowest after PMR compared to SP and PF (3%; 34%; 29%, respectively). Pharyngeal flap procedures resulted in the best speech outcomes.
Conclusions: PMR results in fewer postoperative complications in terms of OSA and achieves a satisfactory reduction in hypernasal speech. PF procedure carries a higher risk of developing OSA postoperatively but seems to be superior in the reduction in hypernasality.
研究设计:系统评价。目的:阻塞性睡眠呼吸暂停(OSA)是腭裂修复患者继发性腭咽功能不全手术后可能出现的并发症。各种外科技术用于治疗腭裂修复后继发性腭咽功能不全,但最佳程序仍有争议。这篇综述综述了不同手术方式相关的气道梗阻性结局的发生率。方法:2月1日按照PRISMA指南进行系统检索,并在PROSPERO上注册(CRD42022299715)。以下数据库被审查:Medline, EMBASE, Web of Science,谷歌Scholar和Cochrane Library数据库。包括腭裂修复后儿童腭咽手术后OSA发生数据的研究。包括综合征性腭裂患者的非英语文章和研究被排除在外。结果:28篇文章符合纳入标准。外科手术分为三组:咽瓣手术(PF)、咽括约肌成形术(SP)和腭肌复位(PMR)。与SP和PF相比,PMR术后OSA的发生率和OSA症状最低(3%;34%;分别为29%)。咽瓣手术的效果最好。结论:PMR减少了OSA的术后并发症,并达到了令人满意的减少高鼻音的效果。PF手术术后发生OSA的风险较高,但在减少鼻音过高方面似乎更优越。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


