Unadjusted Unplanned 30-Day Hospital Readmission Rates are Not a Useful Quality Measure for Planned or Urgent Orthopaedic Inpatient Care: A Retrospective Cohort Study.
Samuel F Turner, Vijay Badial, Reece Barter, Edward Hayter, Raymond E Anakwe
{"title":"Unadjusted Unplanned 30-Day Hospital Readmission Rates are Not a Useful Quality Measure for Planned or Urgent Orthopaedic Inpatient Care: A Retrospective Cohort Study.","authors":"Samuel F Turner, Vijay Badial, Reece Barter, Edward Hayter, Raymond E Anakwe","doi":"10.2106/JBJS.OA.24.00237","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We examined the number of patients who experienced an unplanned hospital readmission following an episode of inpatient care in a tertiary level trauma and orthopaedic service, the reasons for readmission and whether these reasons related to lapses in care, care and service delivery problems, and missed healthcare intervention opportunities and whether they were or should have been prevented and anticipated. We hypothesized that most 30-day readmissions would be unrelated to the original complaint and admission, and the reasons for readmission would not be truly avoidable or attributable to the index hospital admission. We further hypothesized that socioeconomic factors would be predictive of the likelihood of unplanned hospital readmission within 30 days of hospital discharge.</p><p><strong>Methods: </strong>Over a 5-year study period, we identified all adult patients discharged from our unit and those who had an unplanned readmission within 30 days of discharge. We evaluated the reasons for readmission and assessed the impact of socioeconomic deprivation and social determinants of health on the likelihood of unplanned 30-day readmission using multivariable logistic regression.</p><p><strong>Results: </strong>Fifteen thousand three hundred thirteen patients were discharged from our unit over the study period. 690 patients (4.5%) were readmitted within 30 days of discharge as an unplanned episode of care. 58.4% of unplanned readmissions were directly related to the index admission, but only 9% of readmissions were preventable. The single most frequent reason for readmission was an unrelated noninfective medical complaint, 244 patients (35.4%). Social determinants of health influenced the risk of an unplanned readmission, particularly the Index of Multiple Deprivation and the subdomains related to housing, the living environment, social services, and support.</p><p><strong>Conclusions: </strong>The 30-day readmission rate as a marker of quality for inpatient care should be questioned. It is not useful as an unadjusted metric and can be misleading. Adjusting for socioeconomic influences, preventability of readmissions, and missed opportunities to improve whole health may improve its usefulness.</p><p><strong>Level of evidence: </strong>Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 2","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020703/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.24.00237","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We examined the number of patients who experienced an unplanned hospital readmission following an episode of inpatient care in a tertiary level trauma and orthopaedic service, the reasons for readmission and whether these reasons related to lapses in care, care and service delivery problems, and missed healthcare intervention opportunities and whether they were or should have been prevented and anticipated. We hypothesized that most 30-day readmissions would be unrelated to the original complaint and admission, and the reasons for readmission would not be truly avoidable or attributable to the index hospital admission. We further hypothesized that socioeconomic factors would be predictive of the likelihood of unplanned hospital readmission within 30 days of hospital discharge.
Methods: Over a 5-year study period, we identified all adult patients discharged from our unit and those who had an unplanned readmission within 30 days of discharge. We evaluated the reasons for readmission and assessed the impact of socioeconomic deprivation and social determinants of health on the likelihood of unplanned 30-day readmission using multivariable logistic regression.
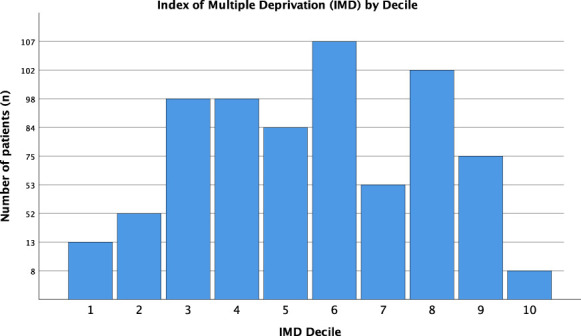
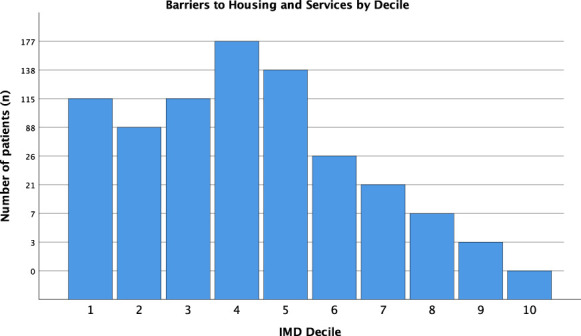
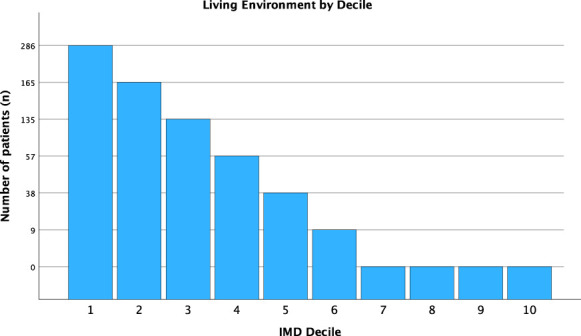
Results: Fifteen thousand three hundred thirteen patients were discharged from our unit over the study period. 690 patients (4.5%) were readmitted within 30 days of discharge as an unplanned episode of care. 58.4% of unplanned readmissions were directly related to the index admission, but only 9% of readmissions were preventable. The single most frequent reason for readmission was an unrelated noninfective medical complaint, 244 patients (35.4%). Social determinants of health influenced the risk of an unplanned readmission, particularly the Index of Multiple Deprivation and the subdomains related to housing, the living environment, social services, and support.
Conclusions: The 30-day readmission rate as a marker of quality for inpatient care should be questioned. It is not useful as an unadjusted metric and can be misleading. Adjusting for socioeconomic influences, preventability of readmissions, and missed opportunities to improve whole health may improve its usefulness.
Level of evidence: Level III. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


