Shiwani Kamath, Abdullah Jahangir, Salim Daouk, Houssein A Youness
{"title":"Mediastinal lymph node cryobiopsy guided by endobronchial ultrasound: a comprehensive review of methods and outcomes.","authors":"Shiwani Kamath, Abdullah Jahangir, Salim Daouk, Houssein A Youness","doi":"10.21037/med-24-39","DOIUrl":null,"url":null,"abstract":"<p><p>Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is the preferred initial method to diagnose and stage non-small cell lung cancer. EBUS-guided transbronchial cryobiopsy (EBUS-TBC) is a newer technique with the potential to address the limitations of EBUS-TBNA. Only a few studies have explored this technique and compared its diagnostic yield to that of EBUS-TBNA. This review aims to summarize the existing literature and provide insights into the optimal yield and technique for performing EBUS-TBC. A comprehensive search of the PubMed database was conducted for studies published up to May 2024 related to EBUS-TBC. The PICO framework (Participants, Intervention, Comparison, and Outcome) was used to evaluate the diagnostic yield, techniques employed, and associated complications. Eleven studies involving 857 patients were identified. In these trials, EBUS-TBC was performed after EBUS-TBNA at the same lymph node station. Techniques varied among bronchoscopists, with most procedures conducted under moderate sedation. The TBNA needle sizes ranged from 19G to 22G. Three trials used a needle knife for the initial mucosal incision, while others utilized the initial puncture site for cryoprobe insertion. Nine studies employed a 1.1-mm Erbe cryoprobe, with a median freezing time of 4 seconds (range, 3-7 seconds). The overall diagnostic yield of EBUS-TBC was 91.9%, compared to 76.6% for EBUS-TBNA alone, with EBUS-TBC yielding larger specimens. Mild bleeding was the most common complication reported. The addition of EBUS-TBC to EBUS-TBNA enhances the diagnostic yield without significantly increasing complications. The larger biopsy samples obtained can be particularly valuable for next-generation sequencing in lung cancer and for improving diagnostic accuracy in benign diseases and rare malignancies like lymphoma.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"9 ","pages":"6"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982995/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-24-39","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
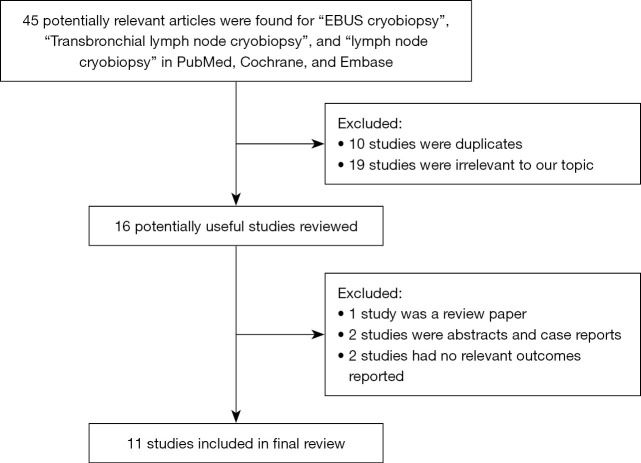
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is the preferred initial method to diagnose and stage non-small cell lung cancer. EBUS-guided transbronchial cryobiopsy (EBUS-TBC) is a newer technique with the potential to address the limitations of EBUS-TBNA. Only a few studies have explored this technique and compared its diagnostic yield to that of EBUS-TBNA. This review aims to summarize the existing literature and provide insights into the optimal yield and technique for performing EBUS-TBC. A comprehensive search of the PubMed database was conducted for studies published up to May 2024 related to EBUS-TBC. The PICO framework (Participants, Intervention, Comparison, and Outcome) was used to evaluate the diagnostic yield, techniques employed, and associated complications. Eleven studies involving 857 patients were identified. In these trials, EBUS-TBC was performed after EBUS-TBNA at the same lymph node station. Techniques varied among bronchoscopists, with most procedures conducted under moderate sedation. The TBNA needle sizes ranged from 19G to 22G. Three trials used a needle knife for the initial mucosal incision, while others utilized the initial puncture site for cryoprobe insertion. Nine studies employed a 1.1-mm Erbe cryoprobe, with a median freezing time of 4 seconds (range, 3-7 seconds). The overall diagnostic yield of EBUS-TBC was 91.9%, compared to 76.6% for EBUS-TBNA alone, with EBUS-TBC yielding larger specimens. Mild bleeding was the most common complication reported. The addition of EBUS-TBC to EBUS-TBNA enhances the diagnostic yield without significantly increasing complications. The larger biopsy samples obtained can be particularly valuable for next-generation sequencing in lung cancer and for improving diagnostic accuracy in benign diseases and rare malignancies like lymphoma.
支气管超声引导下经支气管针吸(EBUS-TBNA)是诊断和分期非小细胞肺癌的首选初始方法。ebus引导下的经支气管冷冻活检(EBUS-TBC)是一种较新的技术,有可能解决EBUS-TBNA的局限性。只有少数研究探索了这种技术,并将其诊断率与EBUS-TBNA进行了比较。这篇综述旨在总结现有的文献,并对进行EBUS-TBC的最佳收率和技术提供见解。对PubMed数据库进行了全面搜索,以获取截至2024年5月发表的与EBUS-TBC相关的研究。PICO框架(参与者、干预、比较和结果)用于评估诊断率、采用的技术和相关并发症。11项研究涉及857例患者。在这些试验中,在同一淋巴结站进行EBUS-TBNA后进行EBUS-TBC。支气管镜医师的技术各不相同,大多数手术在适度镇静下进行。TBNA针径为19G ~ 22G。三个试验使用针刀进行初始粘膜切口,而其他试验使用初始穿刺部位进行冷冻探针插入。9项研究采用1.1 mm Erbe冷冻探针,中位冷冻时间为4秒(范围3-7秒)。EBUS-TBC的总体诊断率为91.9%,而单独的EBUS-TBNA的诊断率为76.6%,EBUS-TBC产生更大的标本。轻度出血是最常见的并发症。在EBUS-TBNA的基础上添加EBUS-TBC可提高诊断率,但不会显著增加并发症。获得的较大活检样本对于肺癌的下一代测序以及提高良性疾病和罕见恶性肿瘤(如淋巴瘤)的诊断准确性尤其有价值。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


