Michael Hermsen, Patrick G Lyons, Govind Persad, Alice F Bewley, Chengsheng Mao, Kaveri Chhikara, Anoop Mayampurath, Matthew Churpek, Monica E Peek, Yuan Luo, William F Parker
{"title":"Age and Saving Lives in Crisis Standards of Care: A Multicenter Cohort Study of Triage Score Prognostic Accuracy.","authors":"Michael Hermsen, Patrick G Lyons, Govind Persad, Alice F Bewley, Chengsheng Mao, Kaveri Chhikara, Anoop Mayampurath, Matthew Churpek, Monica E Peek, Yuan Luo, William F Parker","doi":"10.1097/CCE.0000000000001256","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Current protocols to triage life support use scores that are biased and inaccurate.</p><p><strong>Objectives: </strong>To determine if adding age to triage protocols used in disaster scenarios improves the identification of critically ill patients likely to survive.</p><p><strong>Design, setting, and participants: </strong>Observational cohort study from March 1, 2020, to March 1, 2022, at 22 hospitals in three networks, divided into derivation (12 hospitals) and validation cohorts (ten hospitals). Participants were critically ill adults (90% COVID-19 positive) who would have needed life support during an overwhelming case surge. Life support was defined as vasoactive medications for shock, invasive or noninvasive mechanical ventilation, or oxygen therapy with Pao2/Fio2 less than 200.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was death in the intensive care unit. We fit logistic regression models using a modified Sequential Organ Failure Assessment (SOFA) score with and without age in the derivation cohort and assessed predictive performance in the validation cohort using area under the receiver operating characteristic curves (AUCs) and compared observed and predicted mortality.</p><p><strong>Results: </strong>The final analysis contained 7,660 patients with 16,711 life-support episodes. In the validation cohort, the AUC for age plus SOFA was significantly higher than the AUC for SOFA alone (0.66 vs. 0.54; p < 0.001). SOFA score substantially overpredicted mortality (13% predicted vs. 5% observed) for younger patients (< 40 yr) and underestimated mortality (14% predicted vs. 31% observed) for older patients (> 80 yr). In contrast, age plus SOFA had good calibration overall and across age groups. The addition of age improved but did not eliminate differences between observed and predicted mortality across racial-ethnic groups.</p><p><strong>Conclusions and relevance: </strong>Age-inclusive triage better identifies ICU survivors than SOFA alone and is more equitable. Incorporating age into prioritization algorithms could save more lives in a crisis scenario.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 5","pages":"e1256"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12074069/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001256","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Current protocols to triage life support use scores that are biased and inaccurate.
Objectives: To determine if adding age to triage protocols used in disaster scenarios improves the identification of critically ill patients likely to survive.
Design, setting, and participants: Observational cohort study from March 1, 2020, to March 1, 2022, at 22 hospitals in three networks, divided into derivation (12 hospitals) and validation cohorts (ten hospitals). Participants were critically ill adults (90% COVID-19 positive) who would have needed life support during an overwhelming case surge. Life support was defined as vasoactive medications for shock, invasive or noninvasive mechanical ventilation, or oxygen therapy with Pao2/Fio2 less than 200.
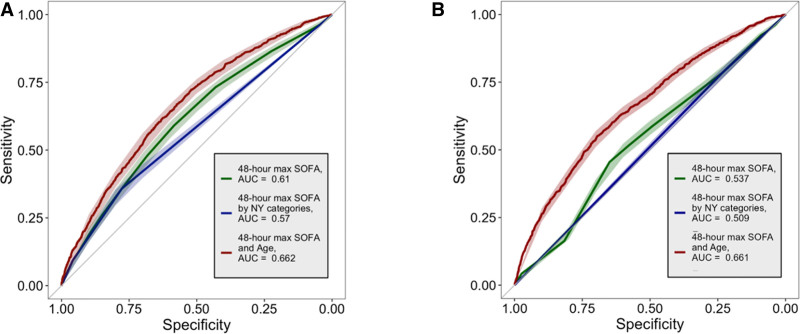
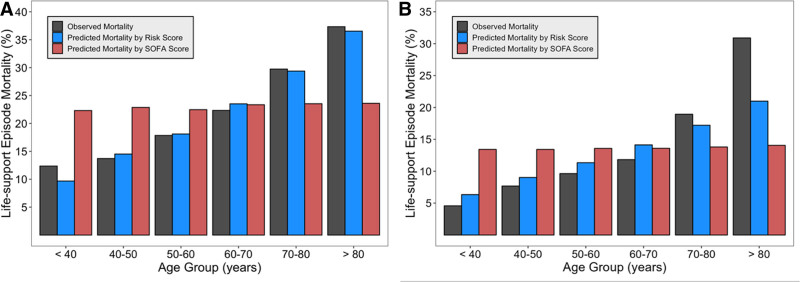
Main outcomes and measures: The primary outcome was death in the intensive care unit. We fit logistic regression models using a modified Sequential Organ Failure Assessment (SOFA) score with and without age in the derivation cohort and assessed predictive performance in the validation cohort using area under the receiver operating characteristic curves (AUCs) and compared observed and predicted mortality.
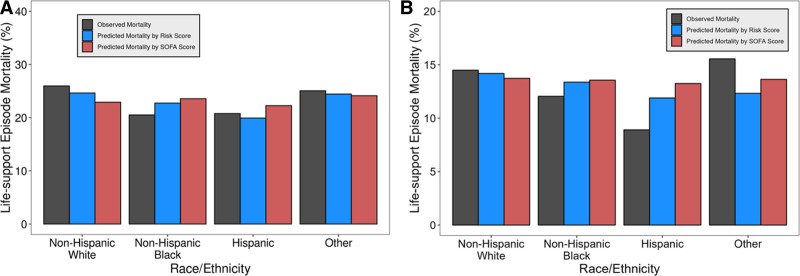
Results: The final analysis contained 7,660 patients with 16,711 life-support episodes. In the validation cohort, the AUC for age plus SOFA was significantly higher than the AUC for SOFA alone (0.66 vs. 0.54; p < 0.001). SOFA score substantially overpredicted mortality (13% predicted vs. 5% observed) for younger patients (< 40 yr) and underestimated mortality (14% predicted vs. 31% observed) for older patients (> 80 yr). In contrast, age plus SOFA had good calibration overall and across age groups. The addition of age improved but did not eliminate differences between observed and predicted mortality across racial-ethnic groups.
Conclusions and relevance: Age-inclusive triage better identifies ICU survivors than SOFA alone and is more equitable. Incorporating age into prioritization algorithms could save more lives in a crisis scenario.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


