{"title":"Predictive factors at emergency department admission for a complicated course of acute pancreatitis.","authors":"Fatih Acehan, Ihsan Ateş, Nisbet Yilmaz","doi":"10.14744/tjtes.2025.05070","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute pancreatitis (AP) is a condition frequently encountered by emergency department (ED) physicians, presenting with a spectrum of severity ranging from a mild, uncomplicated form to a severe, potentially fatal one. This study aimed to identify ED admission parameters that could predict a complicated disease course in patients with AP.</p><p><strong>Methods: </strong>Patients consecutively diagnosed with AP between 2010 and 2018 were included in the study and categorized into complicated and uncomplicated AP groups based on disease progression. Various clinical and laboratory characteristics at ED admission were compared between the two groups, and independent risk factors for complicated AP were identified. Complicated AP was de-fined as the development of any of the following during hospitalization: death, severe disease, necrosis, late peripancreatic or vascular complications, and pancreatic/peripancreatic or major extrapancreatic infections.</p><p><strong>Results: </strong>Of the 511 patients included in the study, 74 (14.5%) were classified into the complicated AP group. At ED admission, recurrent AP, alcoholic etiology, pleural effusion, systemic inflammatory response syndrome, and calcium levels were identified as independent risk factors for complicated AP. The area under the curve for the combination of these five predictors for complicated AP was 0.857 (95% confidence interval: 0.810-0.904), significantly higher than that of existing scoring systems.</p><p><strong>Conclusion: </strong>Using five simple parameters, the development of complicated AP was successfully predicted. These parameters should be considered in the development of new scoring systems to identify patients at risk for clinically severe outcomes in AP.</p>","PeriodicalId":94263,"journal":{"name":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","volume":"31 4","pages":"341-349"},"PeriodicalIF":1.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12000972/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/tjtes.2025.05070","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute pancreatitis (AP) is a condition frequently encountered by emergency department (ED) physicians, presenting with a spectrum of severity ranging from a mild, uncomplicated form to a severe, potentially fatal one. This study aimed to identify ED admission parameters that could predict a complicated disease course in patients with AP.
Methods: Patients consecutively diagnosed with AP between 2010 and 2018 were included in the study and categorized into complicated and uncomplicated AP groups based on disease progression. Various clinical and laboratory characteristics at ED admission were compared between the two groups, and independent risk factors for complicated AP were identified. Complicated AP was de-fined as the development of any of the following during hospitalization: death, severe disease, necrosis, late peripancreatic or vascular complications, and pancreatic/peripancreatic or major extrapancreatic infections.
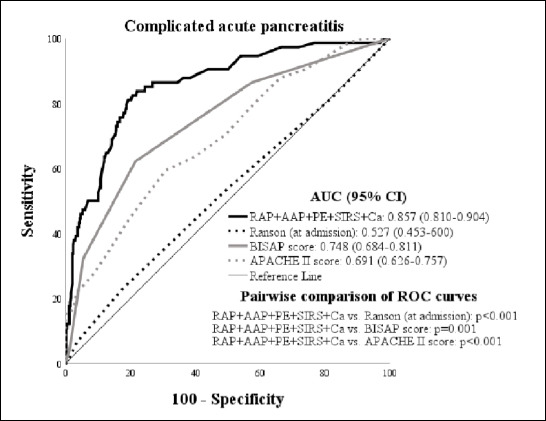
Results: Of the 511 patients included in the study, 74 (14.5%) were classified into the complicated AP group. At ED admission, recurrent AP, alcoholic etiology, pleural effusion, systemic inflammatory response syndrome, and calcium levels were identified as independent risk factors for complicated AP. The area under the curve for the combination of these five predictors for complicated AP was 0.857 (95% confidence interval: 0.810-0.904), significantly higher than that of existing scoring systems.
Conclusion: Using five simple parameters, the development of complicated AP was successfully predicted. These parameters should be considered in the development of new scoring systems to identify patients at risk for clinically severe outcomes in AP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


