Introducing an on-site Helicopter Emergency Medical Service (HEMS) physician at the Emergency Medical Communication Centre - implications for dispatch precision at a Norwegian HEMS base.
Ole Erik Ulvin, Oddvar Uleberg, Andreas Asheim, Helge Haugland
{"title":"Introducing an on-site Helicopter Emergency Medical Service (HEMS) physician at the Emergency Medical Communication Centre - implications for dispatch precision at a Norwegian HEMS base.","authors":"Ole Erik Ulvin, Oddvar Uleberg, Andreas Asheim, Helge Haugland","doi":"10.1186/s13049-025-01396-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dispatch precision of Helicopter Emergency Medical Services (HEMS) is a key topic in prehospital research. In Norway, the combined role of the HEMS physician on-call and the Emergency Medical Communication Centre (EMCC) physician has been challenged. This study aimed to evaluate the impact on HEMS dispatch precision by transferring the medical decision-making from an on-call HEMS physician to an on-site HEMS physician in the EMCC.</p><p><strong>Methods: </strong>In this quasi-experimental study, a HEMS physician was on-site in Trondheim EMCC during defined working hours from February 1st through July 5th, 2024. When on-site, the decision to dispatch Trondheim HEMS was made by this EMCC physician. Primary outcome was unnecessary HEMS dispatches, i.e. missions where neither advanced treatment nor logistical contributions were provided following HEMS dispatch. Secondary outcomes were HEMS alarm and activation time, rejected HEMS missions and National Advisory Committee for Aeronautics (NACA)-scores of encountered HEMS patients. Outcomes were analysed by difference-in-differences analyses.</p><p><strong>Results: </strong>785 HEMS missions were included in the analyses. There was no significant difference in the risk of an unnecessary mission (percentage point risk difference [RD] 5.6, 95% confidence interval [CI] -7.4-18.6) or the proportion of patients with NACA scores of 4 or higher (RD -5.8, 95% CI -17.9-6.3) following the intervention.</p><p><strong>Conclusion: </strong>We found no evidence of increased HEMS dispatch precision, measured by the proportion of missions without medical or logistical contributions, when transferring the medical decision regarding HEMS dispatch from the HEMS physician on-call to an on-site EMCC physician in this study.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"80"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12057114/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01396-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Dispatch precision of Helicopter Emergency Medical Services (HEMS) is a key topic in prehospital research. In Norway, the combined role of the HEMS physician on-call and the Emergency Medical Communication Centre (EMCC) physician has been challenged. This study aimed to evaluate the impact on HEMS dispatch precision by transferring the medical decision-making from an on-call HEMS physician to an on-site HEMS physician in the EMCC.
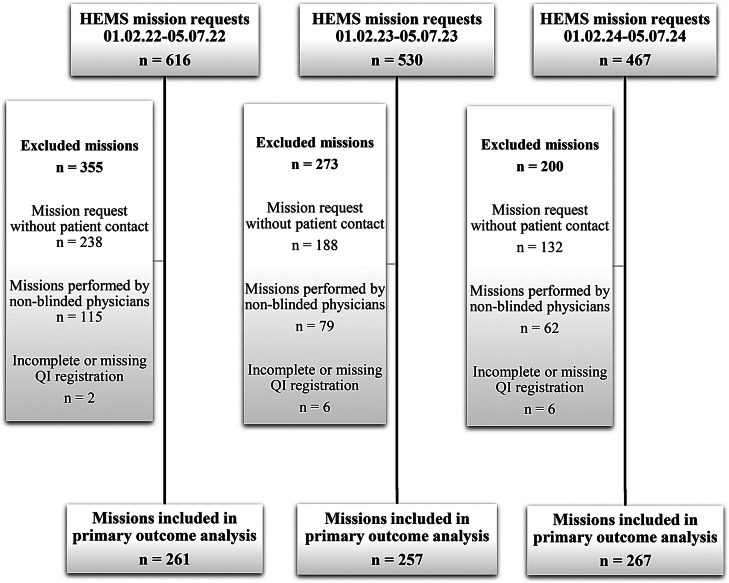
Methods: In this quasi-experimental study, a HEMS physician was on-site in Trondheim EMCC during defined working hours from February 1st through July 5th, 2024. When on-site, the decision to dispatch Trondheim HEMS was made by this EMCC physician. Primary outcome was unnecessary HEMS dispatches, i.e. missions where neither advanced treatment nor logistical contributions were provided following HEMS dispatch. Secondary outcomes were HEMS alarm and activation time, rejected HEMS missions and National Advisory Committee for Aeronautics (NACA)-scores of encountered HEMS patients. Outcomes were analysed by difference-in-differences analyses.
Results: 785 HEMS missions were included in the analyses. There was no significant difference in the risk of an unnecessary mission (percentage point risk difference [RD] 5.6, 95% confidence interval [CI] -7.4-18.6) or the proportion of patients with NACA scores of 4 or higher (RD -5.8, 95% CI -17.9-6.3) following the intervention.
Conclusion: We found no evidence of increased HEMS dispatch precision, measured by the proportion of missions without medical or logistical contributions, when transferring the medical decision regarding HEMS dispatch from the HEMS physician on-call to an on-site EMCC physician in this study.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


