Feyza Erenler, Benjamin Katcher, Van Phan, Knarik Arkun, Mina G Safain
{"title":"Thyroid-Stimulating Hormone/Growth Hormone Cosecreting Pituitary Adenoma With Normal Thyroid-Stimulating Hormone Level.","authors":"Feyza Erenler, Benjamin Katcher, Van Phan, Knarik Arkun, Mina G Safain","doi":"10.1210/jcemcr/luaf063","DOIUrl":null,"url":null,"abstract":"<p><p>Thyroid-stimulating hormone (TSH; thyrotropin) adenoma is a rare pituitary tumor that can be missed due to its subtle symptoms. We are reporting a 67-year-old man with history of ventricular fibrillation on amiodarone who presented with acute headache and right third cranial nerve palsy. His computed tomography (CT) scan revealed a 2.2-cm suprasellar mass, consistent with pituitary apoplexy, and he underwent pituitary tumor resection. Preoperational hormonal workup revealed TSH 0.25 mIU/mL (0.25 IU/L) (normal reference range: 0.35-4.94 mIU/mL; 0.35-4.94 IU/L), free thyroxine (T4) 3.17 ng/dL (40.80 pmol/L) (normal reference range: 0.7-1.48 ng/dL; 9.78-19.05 pmol/L), and total triiodothyronine (T3) 91 ng/dL (140 nmol/L) (normal reference range: 58-159 ng/dL; 89-244 nmol/L). Initial differential diagnoses included TSH-producing pituitary adenoma (TSH-oma) and amiodarone-induced thyrotoxicosis. His free T4 declined significantly postoperatively, favoring a TSH-oma diagnosis. The pathology report showed a TSH and growth hormone (GH) cosecreting adenoma. Furthermore, he had a normal thyroid uptake scan, as well as negative thyroid antibodies, making primary thyroid diseases less likely. A high free T4 with normal TSH 3 years ago, prior to the start of amiodarone, suggested a long disease duration. This case demonstrates challenges in diagnosing TSH-oma, especially in patients with normal TSH and concurrent amiodarone use.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"3 5","pages":"luaf063"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11986576/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luaf063","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
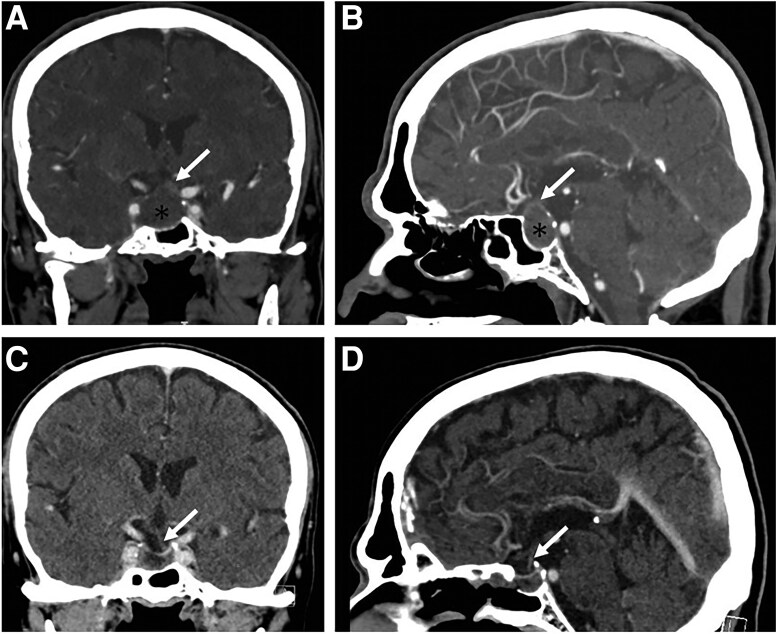
Thyroid-stimulating hormone (TSH; thyrotropin) adenoma is a rare pituitary tumor that can be missed due to its subtle symptoms. We are reporting a 67-year-old man with history of ventricular fibrillation on amiodarone who presented with acute headache and right third cranial nerve palsy. His computed tomography (CT) scan revealed a 2.2-cm suprasellar mass, consistent with pituitary apoplexy, and he underwent pituitary tumor resection. Preoperational hormonal workup revealed TSH 0.25 mIU/mL (0.25 IU/L) (normal reference range: 0.35-4.94 mIU/mL; 0.35-4.94 IU/L), free thyroxine (T4) 3.17 ng/dL (40.80 pmol/L) (normal reference range: 0.7-1.48 ng/dL; 9.78-19.05 pmol/L), and total triiodothyronine (T3) 91 ng/dL (140 nmol/L) (normal reference range: 58-159 ng/dL; 89-244 nmol/L). Initial differential diagnoses included TSH-producing pituitary adenoma (TSH-oma) and amiodarone-induced thyrotoxicosis. His free T4 declined significantly postoperatively, favoring a TSH-oma diagnosis. The pathology report showed a TSH and growth hormone (GH) cosecreting adenoma. Furthermore, he had a normal thyroid uptake scan, as well as negative thyroid antibodies, making primary thyroid diseases less likely. A high free T4 with normal TSH 3 years ago, prior to the start of amiodarone, suggested a long disease duration. This case demonstrates challenges in diagnosing TSH-oma, especially in patients with normal TSH and concurrent amiodarone use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


