Sejal M Bhavsar, Erica B Casella, Maureen Kim, Patrick Lake, Sabrina Malik, Kaitlyn Philips, Pooja Shah, Shevaitha T Shyamalan, Stefan Hagmann
{"title":"Reduction of Vancomycin Use in a Neonatal Intensive Care Unit: A Quality Improvement Project.","authors":"Sejal M Bhavsar, Erica B Casella, Maureen Kim, Patrick Lake, Sabrina Malik, Kaitlyn Philips, Pooja Shah, Shevaitha T Shyamalan, Stefan Hagmann","doi":"10.1097/pq9.0000000000000810","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Late-onset sepsis (LOS) is a common cause of neonatal morbidity and mortality. Professional organizations recommend avoiding empiric vancomycin use in neonates without risk factors for methicillin-resistant <i>Staphylococcus aureus</i> infection. We aimed to reduce the mean vancomycin antibiotic utilization rate (AUR) by 30% for 12 months in our neonatal intensive care unit (NICU).</p><p><strong>Methods: </strong>We included neonates admitted to our level-3 NICU from March 15, 2023, to February 29, 2024, with suspected LOS in the intervention period. A multidisciplinary team used the Model for Improvement. Interventions tested using plan-do-study-act cycles included provider education, clinical practice guideline (CPG) implementation, and prospective audit with feedback (PAF). The outcome measure was the mean vancomycin AUR measured in days of therapy per 1,000 patients days, plotted monthly and analyzed for special cause variation. The process measure was CPG adherence. We tracked balancing measures related to morbidity and mortality.</p><p><strong>Results: </strong>During the intervention period, 50 neonates underwent LOS evaluations. The mean vancomycin AUR decreased by 37.1%, from 27 to 17 days of therapy per 1,000 patient days, and was sustained postintervention. CPG adherence was 96%. Three neonates required changing from oxacillin to vancomycin for coagulase-negative staphylococci bacteremia (n = 2) and urinary tract infection (n = 1). There were no drug-related morbidity or sepsis-related mortality events.</p><p><strong>Conclusions: </strong>This quality improvement project allowed a safe, rapid and sustained reduction of NICU-wide vancomycin use. Provider education, CPG implementation, and PAF were critical to optimizing empiric antibiotic management.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"10 3","pages":"e810"},"PeriodicalIF":1.1000,"publicationDate":"2025-05-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12052236/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000810","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Late-onset sepsis (LOS) is a common cause of neonatal morbidity and mortality. Professional organizations recommend avoiding empiric vancomycin use in neonates without risk factors for methicillin-resistant Staphylococcus aureus infection. We aimed to reduce the mean vancomycin antibiotic utilization rate (AUR) by 30% for 12 months in our neonatal intensive care unit (NICU).
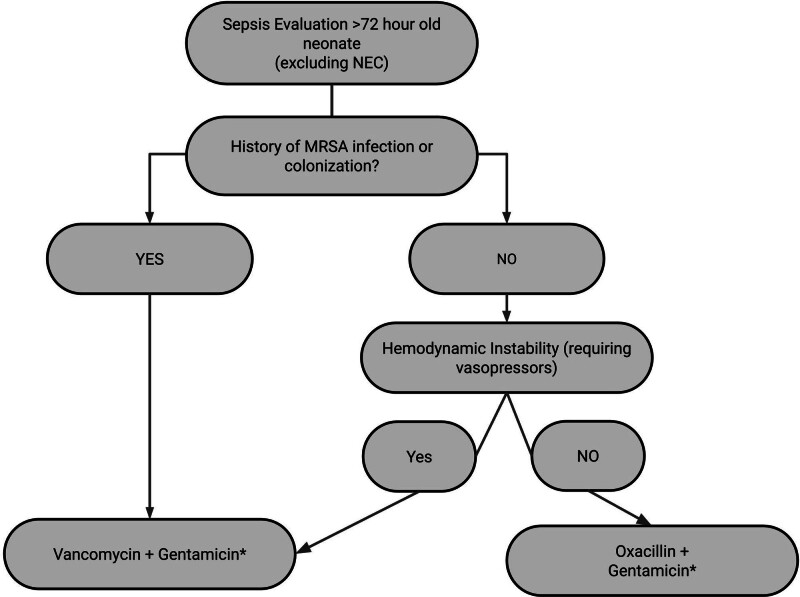
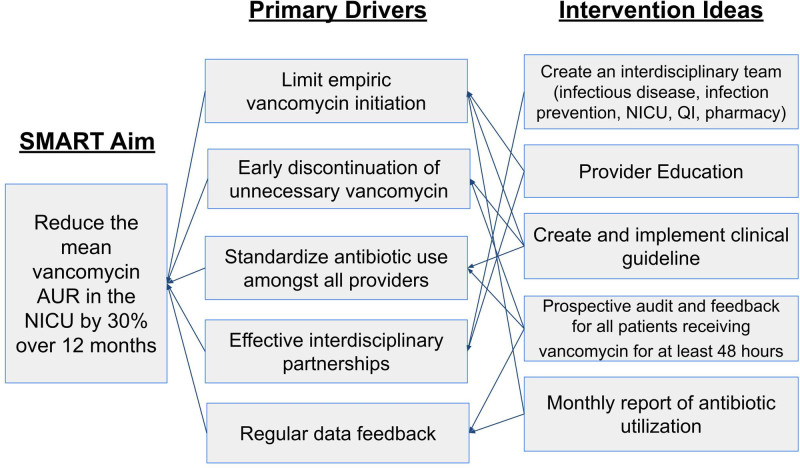
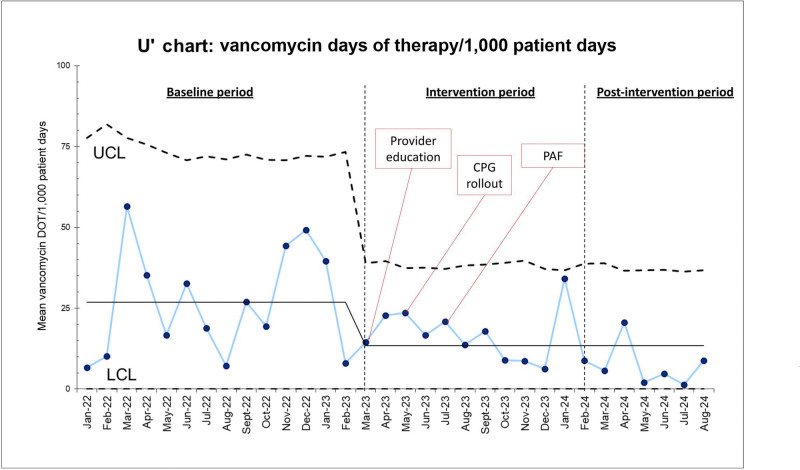
Methods: We included neonates admitted to our level-3 NICU from March 15, 2023, to February 29, 2024, with suspected LOS in the intervention period. A multidisciplinary team used the Model for Improvement. Interventions tested using plan-do-study-act cycles included provider education, clinical practice guideline (CPG) implementation, and prospective audit with feedback (PAF). The outcome measure was the mean vancomycin AUR measured in days of therapy per 1,000 patients days, plotted monthly and analyzed for special cause variation. The process measure was CPG adherence. We tracked balancing measures related to morbidity and mortality.
Results: During the intervention period, 50 neonates underwent LOS evaluations. The mean vancomycin AUR decreased by 37.1%, from 27 to 17 days of therapy per 1,000 patient days, and was sustained postintervention. CPG adherence was 96%. Three neonates required changing from oxacillin to vancomycin for coagulase-negative staphylococci bacteremia (n = 2) and urinary tract infection (n = 1). There were no drug-related morbidity or sepsis-related mortality events.
Conclusions: This quality improvement project allowed a safe, rapid and sustained reduction of NICU-wide vancomycin use. Provider education, CPG implementation, and PAF were critical to optimizing empiric antibiotic management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


