Jessica L Fairley, Dylan Hansen, Susanna Proudman, Joanne Sahhar, Gene-Siew Ngian, Diane Apostolopoulos, Jennifer Walker, Lauren V Host, Wendy Stevens, Mandana Nikpour, Laura Ross
{"title":"The Prognostic and Functional Impact of Multimorbidity in Systemic Sclerosis.","authors":"Jessica L Fairley, Dylan Hansen, Susanna Proudman, Joanne Sahhar, Gene-Siew Ngian, Diane Apostolopoulos, Jennifer Walker, Lauren V Host, Wendy Stevens, Mandana Nikpour, Laura Ross","doi":"10.1002/acr2.70034","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Our objective was to define the frequency and impact of multimorbidity in systemic sclerosis (SSc).</p><p><strong>Method: </strong>Australian Scleroderma Cohort Study participants meeting American College of Rheumatology/EULAR criteria were included. Charlson Comorbidity Index scores were calculated at each visit, with multimorbidity defined as scores ≥4. Generalized estimating equations were used to model longitudinal data in multivariable models including age, sex, subclass, interstitial lung disease, and pulmonary arterial hypertension status. Survival was analyzed using Cox hazard modeling.</p><p><strong>Results: </strong>Of 2,000 participants, 85% were female, 27% had diffuse SSc, and 20% had multimorbidity. Among those with multimorbidity, key comorbidities were hypertension (81%), dyslipidemia (67%), obstructive lung disease (50%), malignancy (49%), and ischemic heart disease (IHD) (40%). Multimorbidity was associated with worse survival (hazard ratio [HR] 1.57, 95% confidence interval [CI] 1.30-1.91, P < 0.01). Renal disease had the largest impact (HR 2.41, 95% CI 1.46-3.98, P < 0.01), followed by left ventricular dysfunction (HR 1.76, 95% CI 1.21-2.57, P < 0.01), anticoagulation (HR 1.64, 95% CI 1.28-2.08, P < 0.01), and IHD (HR 1.45, 95% CI 1.16-1.80, P < 0.01). In multivariable modeling, multimorbidity was associated with poorer physical function (regression coefficient [RC] +0.17 units, 95% CI 0.13-0.21, P < 0.01). Peripheral vascular disease had the largest impact on physical function (RC +0.26 units, 95% CI 0.18-0.34, P < 0.01), followed by left ventricular dysfunction (RC +0.23 units, 95% CI 0.14-0.33, P = 0.01), IHD (RC +0.22 units, 95% CI 0.17-0.28, P < 0.01), and obstructive lung disease (RC +0.19 units, 95% CI 0.14-0.24, P < 0.01).</p><p><strong>Conclusion: </strong>Multimorbidity occurred in 20% of patients in a large SSc cohort and was an important determinant of both prognosis and physical function. Effective treatment of non-SSc morbidity may improve outcomes for patients with SSc. Graphical Abstract. *p-value <0.05. Multimorbidity defined as Charlson Comorbidity Index scores ≥4.</p><p><strong>Abbreviations: </strong>CI (confidence interval), CKD (chronic kidney disease), COPD (chronic obstructive pulmonary disease), HAQ-DI (health assessment questionnaire disability index), HR (hazard ratio), LVEF (left ventricular ejection fraction), IHD (ischaemic heart disease), HR (hazard ratio), IQR (interquartile range), PVD (peripheral vascular disease), SSc (systemic sclerosis).</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 4","pages":"e70034"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12012261/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Our objective was to define the frequency and impact of multimorbidity in systemic sclerosis (SSc).
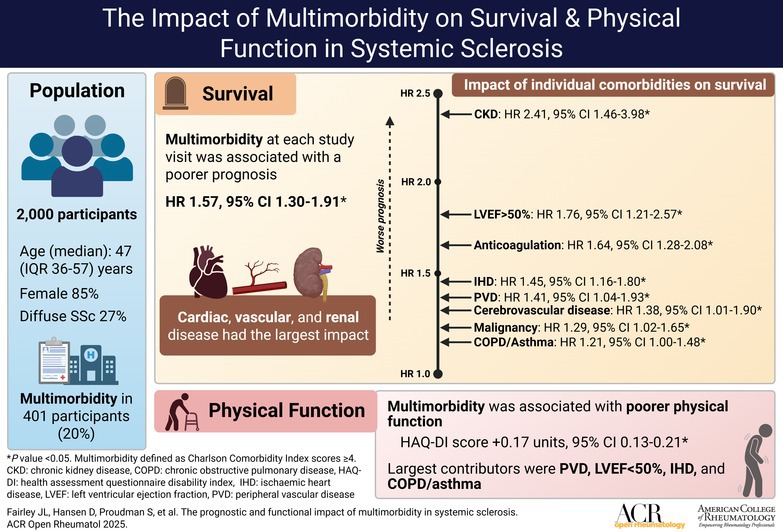
Method: Australian Scleroderma Cohort Study participants meeting American College of Rheumatology/EULAR criteria were included. Charlson Comorbidity Index scores were calculated at each visit, with multimorbidity defined as scores ≥4. Generalized estimating equations were used to model longitudinal data in multivariable models including age, sex, subclass, interstitial lung disease, and pulmonary arterial hypertension status. Survival was analyzed using Cox hazard modeling.
Results: Of 2,000 participants, 85% were female, 27% had diffuse SSc, and 20% had multimorbidity. Among those with multimorbidity, key comorbidities were hypertension (81%), dyslipidemia (67%), obstructive lung disease (50%), malignancy (49%), and ischemic heart disease (IHD) (40%). Multimorbidity was associated with worse survival (hazard ratio [HR] 1.57, 95% confidence interval [CI] 1.30-1.91, P < 0.01). Renal disease had the largest impact (HR 2.41, 95% CI 1.46-3.98, P < 0.01), followed by left ventricular dysfunction (HR 1.76, 95% CI 1.21-2.57, P < 0.01), anticoagulation (HR 1.64, 95% CI 1.28-2.08, P < 0.01), and IHD (HR 1.45, 95% CI 1.16-1.80, P < 0.01). In multivariable modeling, multimorbidity was associated with poorer physical function (regression coefficient [RC] +0.17 units, 95% CI 0.13-0.21, P < 0.01). Peripheral vascular disease had the largest impact on physical function (RC +0.26 units, 95% CI 0.18-0.34, P < 0.01), followed by left ventricular dysfunction (RC +0.23 units, 95% CI 0.14-0.33, P = 0.01), IHD (RC +0.22 units, 95% CI 0.17-0.28, P < 0.01), and obstructive lung disease (RC +0.19 units, 95% CI 0.14-0.24, P < 0.01).
Conclusion: Multimorbidity occurred in 20% of patients in a large SSc cohort and was an important determinant of both prognosis and physical function. Effective treatment of non-SSc morbidity may improve outcomes for patients with SSc. Graphical Abstract. *p-value <0.05. Multimorbidity defined as Charlson Comorbidity Index scores ≥4.
目的:我们的目的是确定系统性硬化症(SSc)中多病的频率和影响。方法:纳入符合美国风湿病学会/EULAR标准的澳大利亚硬皮病队列研究参与者。每次就诊时计算Charlson共病指数评分,多重病定义为评分≥4。使用广义估计方程对多变量模型中的纵向数据进行建模,包括年龄、性别、亚类、间质性肺疾病和肺动脉高压状态。采用Cox风险模型分析生存率。结果:在2000名参与者中,85%为女性,27%为弥漫性SSc, 20%为多病。在多病患者中,主要的合并症是高血压(81%)、血脂异常(67%)、阻塞性肺疾病(50%)、恶性肿瘤(49%)和缺血性心脏病(40%)。多病与较差的生存率相关(风险比[HR] 1.57, 95%可信区间[CI] 1.30-1.91, P < 0.01)。肾脏疾病的影响最大(HR 2.41, 95% CI 1.46 ~ 3.98, P < 0.01),其次是左心功能不全(HR 1.76, 95% CI 1.21 ~ 2.57, P < 0.01)、抗凝(HR 1.64, 95% CI 1.28 ~ 2.08, P < 0.01)和IHD (HR 1.45, 95% CI 1.16 ~ 1.80, P < 0.01)。在多变量模型中,多发病与较差的身体功能相关(回归系数[RC] +0.17个单位,95% CI 0.13-0.21, P < 0.01)。外周血管疾病对身体功能的影响最大(RC +0.26单位,95% CI 0.18-0.34, P < 0.01),其次是左心室功能不全(RC +0.23单位,95% CI 0.14-0.33, P = 0.01)、IHD (RC +0.22单位,95% CI 0.17-0.28, P < 0.01)和阻塞性肺疾病(RC +0.19单位,95% CI 0.14-0.24, P < 0.01)。结论:在一个大型SSc队列中,20%的患者出现多病,这是预后和身体功能的重要决定因素。对非SSc发病率的有效治疗可以改善SSc患者的预后。图形抽象。*p值缩写:CI(置信区间)、CKD(慢性肾脏疾病)、COPD(慢性阻塞性肺疾病)、HAQ-DI(健康评估问卷残疾指数)、HR(危险比)、LVEF(左心室射血分数)、IHD(缺血性心脏病)、HR(危险比)、IQR(四分位间距)、PVD(外周血管疾病)、SSc(系统性硬化症)。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


