{"title":"STEPWISE CARDIAC REHABILITATION ADJUSTMENT AFTER EXERCISE-INDUCED IMPLANTABLE CARDIOVERTER DEFIBRILLATOR SHOCK: A CASE REPORT.","authors":"Hidetoshi Yanagi, Harumi Konishi, Saori Yamada, Kazuya Yamamoto, Fumiyuki Otsuka","doi":"10.2340/jrm-cc.v8.42483","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To report an in-hospital cardiac rehabilitation strategy after exercise-induced implantable cardioverter defibrillator shock.</p><p><strong>Case report: </strong>A 72-year-old man with heart failure, peripheral artery disease, a history of percutaneous coronary intervention and coronary artery bypass surgery, exercise-induced ventricular fibrillation, and an implantable cardioverter defibrillator was hospitalised after experiencing recurrent ventricular fibrillation while walking, which triggered implantable cardioverter defibrillator shock. While hospitalised, his medication regimen was adjusted. After passing the 200-m walking test, he started in-hospital cardiac rehabilitation. During cardiopulmonary exercise testing, he experienced non-sustained ventricular tachycardia. Percutaneous coronary intervention was performed to relieve ischaemia; however, ventricular tachycardia recurred during walking, causing another implantable cardioverter defibrillator shock. After further medication adjustments and setting heart rate limits, he gradually resumed cycling and low-intensity resistance exercises, followed by walking, and was subsequently discharged without ventricular tachycardia recurrence.</p><p><strong>Discussion: </strong>Peripheral artery disease-associated pain and increased heart rate may have contributed to ventricular tachycardia. A stepwise exercise programme involving heart rate monitoring and medication therapy adjustments enabled safe exercise resumption after implantable cardioverter defibrillator shock in a patient with multiple comorbidities.</p><p><strong>Conclusion: </strong>This case emphasises the importance of personalised exercise strategies that consider both arrhythmic risk and comorbidities for patients at high risk of exercise-induced arrhythmias.</p>","PeriodicalId":73929,"journal":{"name":"Journal of rehabilitation medicine. Clinical communications","volume":"8 ","pages":"42483"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12016661/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of rehabilitation medicine. Clinical communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2340/jrm-cc.v8.42483","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To report an in-hospital cardiac rehabilitation strategy after exercise-induced implantable cardioverter defibrillator shock.
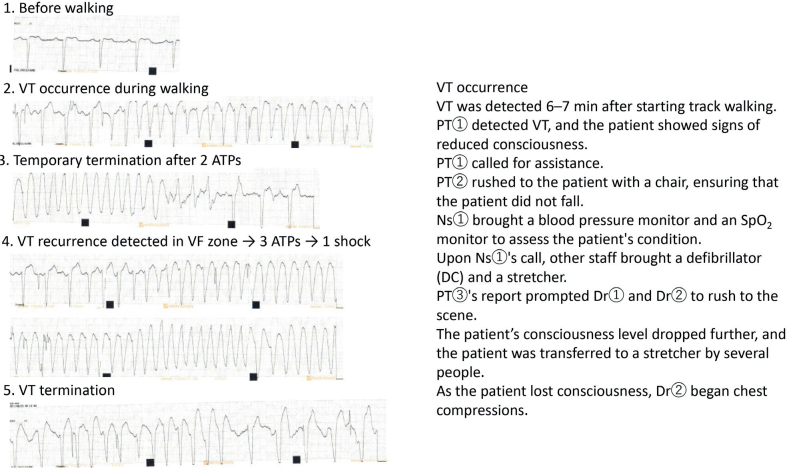
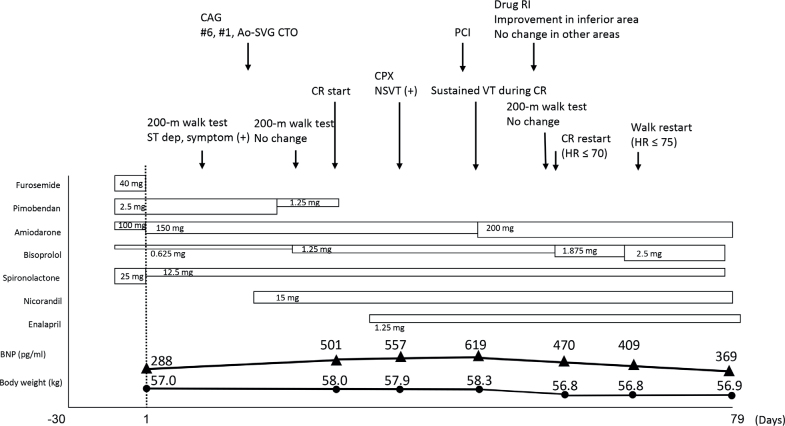
Case report: A 72-year-old man with heart failure, peripheral artery disease, a history of percutaneous coronary intervention and coronary artery bypass surgery, exercise-induced ventricular fibrillation, and an implantable cardioverter defibrillator was hospitalised after experiencing recurrent ventricular fibrillation while walking, which triggered implantable cardioverter defibrillator shock. While hospitalised, his medication regimen was adjusted. After passing the 200-m walking test, he started in-hospital cardiac rehabilitation. During cardiopulmonary exercise testing, he experienced non-sustained ventricular tachycardia. Percutaneous coronary intervention was performed to relieve ischaemia; however, ventricular tachycardia recurred during walking, causing another implantable cardioverter defibrillator shock. After further medication adjustments and setting heart rate limits, he gradually resumed cycling and low-intensity resistance exercises, followed by walking, and was subsequently discharged without ventricular tachycardia recurrence.
Discussion: Peripheral artery disease-associated pain and increased heart rate may have contributed to ventricular tachycardia. A stepwise exercise programme involving heart rate monitoring and medication therapy adjustments enabled safe exercise resumption after implantable cardioverter defibrillator shock in a patient with multiple comorbidities.
Conclusion: This case emphasises the importance of personalised exercise strategies that consider both arrhythmic risk and comorbidities for patients at high risk of exercise-induced arrhythmias.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


