Andreas G Kontopidis, Mark É Czeisler, David H Yoo, Olivia Whittaker, Daniel C Pipilas, Theofanie Mela
{"title":"Noninvasive Impedance Analysis During S-ICD Insertion Provides Justification for Defibrillation Based Testing Deferment.","authors":"Andreas G Kontopidis, Mark É Czeisler, David H Yoo, Olivia Whittaker, Daniel C Pipilas, Theofanie Mela","doi":"10.1111/pace.15199","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Following subcutaneous implantable cardioverter-defibrillator (S-ICD) insertion, induction of ventricular fibrillation (VF) and defibrillation threshold testing (DFT) is the standard of practice to assess system performance. In contrast, DFT testing is not routinely performed after transvenous ICD (T-ICD) insertion, supported by literature that emphasizes negative clinical repercussions and reliability of noninvasive predictors of successful defibrillation. There is a paucity of data for both the trajectory of noninvasive low voltage (LV) impedance measurements at S-ICD insertion through the time of potential DFT testing and for the proximity of LV impedance measurements and high voltage (HV) shock impedance from 65J DFT or 10J testing.</p><p><strong>Objective: </strong>We aim to characterize the trend in LV impedance from initial S-ICD connection (LV T0) to final intraprocedural impedance (LV T4) and to compare LV impedance with HV impedance.</p><p><strong>Methods: </strong>Data from patients who underwent S-ICD implantation between July 2022 and March 2024 were analyzed. LV impedance measurements were collected during implant and HV impedance measurements were collected if 65J DFT/10J testing was performed. Differences in mean impedances at each time point were evaluated using paired t-tests. For those who underwent 10J or 65J DFT testing, LV impedance was compared with HV impedance.</p><p><strong>Results: </strong>The primary analytic sample included 53 patients, with a mean age of 51 ± 15.7 years; 16 (30.2%) were female. LV impedance decreased by a mean of 14.5 ± 9.8 ohms (18.3%; p <0.001) from S-ICD connection (T0) to the final intraprocedural measurement, approximately 60 min postimplant (T4). Among 35 patients who underwent HV testing (65J DFT or 10J), LV impedance at T4 and HV impedance did not differ significantly (1.7 ± 6.3 ohms; p = 0.116).</p><p><strong>Conclusion: </strong>Our findings demonstrate a predictable reduction in LV impedance from S-ICD connection to subsequent intraprocedural measurements. We also found that LV impedance at LV T4, the final intraprocedural measurement, did not significantly differ from contemporaneous HV impedance. Together, these findings indicate that LV impedance at implant can be expected to decline, and that 60-min postimplant LV impedance may reliably approximate HV impedance. Evaluation of circumstances in which LV impedance could influence the decision to perform DFT testing is warranted.</p>","PeriodicalId":54653,"journal":{"name":"Pace-Pacing and Clinical Electrophysiology","volume":" ","pages":"578-586"},"PeriodicalIF":1.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12166533/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pace-Pacing and Clinical Electrophysiology","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.1111/pace.15199","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Following subcutaneous implantable cardioverter-defibrillator (S-ICD) insertion, induction of ventricular fibrillation (VF) and defibrillation threshold testing (DFT) is the standard of practice to assess system performance. In contrast, DFT testing is not routinely performed after transvenous ICD (T-ICD) insertion, supported by literature that emphasizes negative clinical repercussions and reliability of noninvasive predictors of successful defibrillation. There is a paucity of data for both the trajectory of noninvasive low voltage (LV) impedance measurements at S-ICD insertion through the time of potential DFT testing and for the proximity of LV impedance measurements and high voltage (HV) shock impedance from 65J DFT or 10J testing.
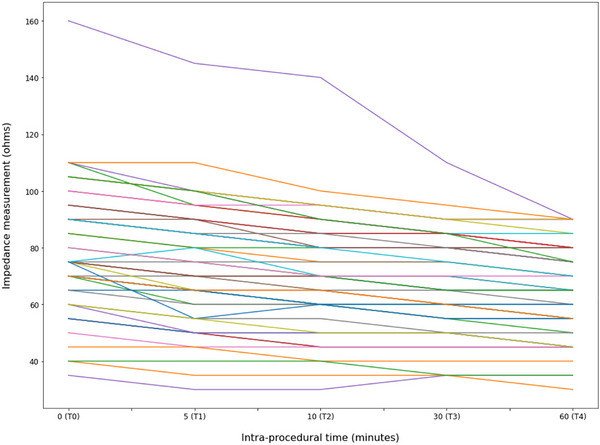
Objective: We aim to characterize the trend in LV impedance from initial S-ICD connection (LV T0) to final intraprocedural impedance (LV T4) and to compare LV impedance with HV impedance.
Methods: Data from patients who underwent S-ICD implantation between July 2022 and March 2024 were analyzed. LV impedance measurements were collected during implant and HV impedance measurements were collected if 65J DFT/10J testing was performed. Differences in mean impedances at each time point were evaluated using paired t-tests. For those who underwent 10J or 65J DFT testing, LV impedance was compared with HV impedance.
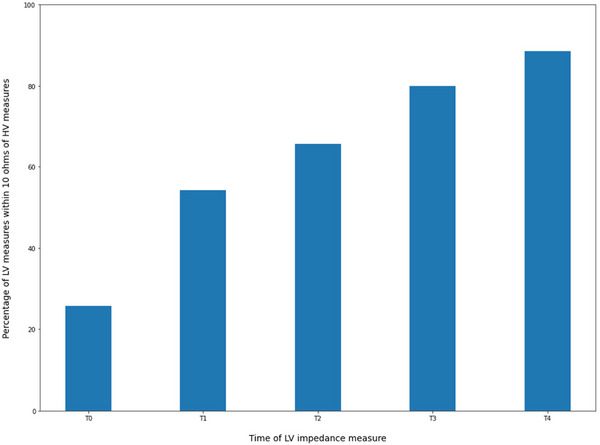
Results: The primary analytic sample included 53 patients, with a mean age of 51 ± 15.7 years; 16 (30.2%) were female. LV impedance decreased by a mean of 14.5 ± 9.8 ohms (18.3%; p <0.001) from S-ICD connection (T0) to the final intraprocedural measurement, approximately 60 min postimplant (T4). Among 35 patients who underwent HV testing (65J DFT or 10J), LV impedance at T4 and HV impedance did not differ significantly (1.7 ± 6.3 ohms; p = 0.116).
Conclusion: Our findings demonstrate a predictable reduction in LV impedance from S-ICD connection to subsequent intraprocedural measurements. We also found that LV impedance at LV T4, the final intraprocedural measurement, did not significantly differ from contemporaneous HV impedance. Together, these findings indicate that LV impedance at implant can be expected to decline, and that 60-min postimplant LV impedance may reliably approximate HV impedance. Evaluation of circumstances in which LV impedance could influence the decision to perform DFT testing is warranted.
期刊介绍:
Pacing and Clinical Electrophysiology (PACE) is the foremost peer-reviewed journal in the field of pacing and implantable cardioversion defibrillation, publishing over 50% of all English language articles in its field, featuring original, review, and didactic papers, and case reports related to daily practice. Articles also include editorials, book reviews, Musings on humane topics relevant to medical practice, electrophysiology (EP) rounds, device rounds, and information concerning the quality of devices used in the practice of the specialty.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


