Perioperative Intravenous Lidocaine Infusion Therapy as an Adjunct to Multimodal Analgesia for Adolescent Idiopathic Scoliosis Surgical Correction: A Double-Blind Randomized Controlled Trial.
Jessica Luo, Nicholas West, Samantha Pang, Aanisah Golam, Erin Adams, Matthias Görges, Roxane R Carr, Firoz Miyanji, Gillian R Lauder
{"title":"Perioperative Intravenous Lidocaine Infusion Therapy as an Adjunct to Multimodal Analgesia for Adolescent Idiopathic Scoliosis Surgical Correction: A Double-Blind Randomized Controlled Trial.","authors":"Jessica Luo, Nicholas West, Samantha Pang, Aanisah Golam, Erin Adams, Matthias Görges, Roxane R Carr, Firoz Miyanji, Gillian R Lauder","doi":"10.1111/pan.15124","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Posterior spinal instrumentation and fusion is a common surgical correction for adolescent idiopathic scoliosis. Preventative multimodal analgesia, including opioids, is required to minimize postoperative pain, but opioids are associated with dose-dependent side effects that may disrupt recovery.</p><p><strong>Aims: </strong>We hypothesized that the addition of 48-h perioperative intravenous lidocaine therapy to a multimodal analgesia regimen would reduce morphine utilization.</p><p><strong>Method: </strong>We conducted a double-blinded randomized controlled trial in 10-19 years old, ASA I-III, undergoing single-stage scoliosis correction. Participants were randomly allocated to the Intervention group (intravenous lidocaine 1 mg kg<sup>-1</sup> bolus at anesthesia start, followed by 2 mg kg<sup>-1</sup> h<sup>-1</sup> infusion for 8 h, followed by 1 mg kg<sup>-1</sup> h<sup>-1</sup> for 40 h) or Control (normal saline). Participants received standardized perioperative multimodal analgesia, including a postoperative morphine infusion with titration rules protocolized to self-reported pain scores. The primary outcome was 48-h morphine utilization; secondary outcomes were median and worst pain scores, and times to first stand, first walk > 15 steps, urinary catheter removal, termination of morphine infusion, and hospital discharge.</p><p><strong>Results: </strong>Data were available from 38 participants: 32 (84%) female; median (IQR) age 16.3 (14.9-17.2) years, with curve magnitude (Cobb angle) 62 (56-70) degrees. The 48-h morphine utilization did not differ between groups: Intervention median (IQR) 0.86 (0.73-1.05) mg kg<sup>-1</sup> versus Control 1.00 (0.77-1.18) mg kg<sup>-1</sup>; median difference -0.11 (95% CI -0.30 to 0.13) mg kg<sup>-1</sup>; p = 0.264. There were similarly no differences in morphine utilization at 12, 24, or 36 h or any secondary outcome, except the first postoperative pain score: Intervention 3/10 (1.75-5) versus Control 5/10 (3-7); median difference -2 (95% CI 0 to -3); p = 0.035. Three cases with mild symptoms of suspected local anesthetic systemic toxicity were observed in the Intervention group.</p><p><strong>Conclusions: </strong>We found no evidence to support the adjunctive use of 48-h perioperative intravenous lidocaine therapy in adolescents undergoing scoliosis correction in which effective multimodal analgesia was adopted.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov identifier: NCT04069169.</p>","PeriodicalId":19745,"journal":{"name":"Pediatric Anesthesia","volume":" ","pages":"552-561"},"PeriodicalIF":1.7000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149479/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/pan.15124","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Posterior spinal instrumentation and fusion is a common surgical correction for adolescent idiopathic scoliosis. Preventative multimodal analgesia, including opioids, is required to minimize postoperative pain, but opioids are associated with dose-dependent side effects that may disrupt recovery.
Aims: We hypothesized that the addition of 48-h perioperative intravenous lidocaine therapy to a multimodal analgesia regimen would reduce morphine utilization.
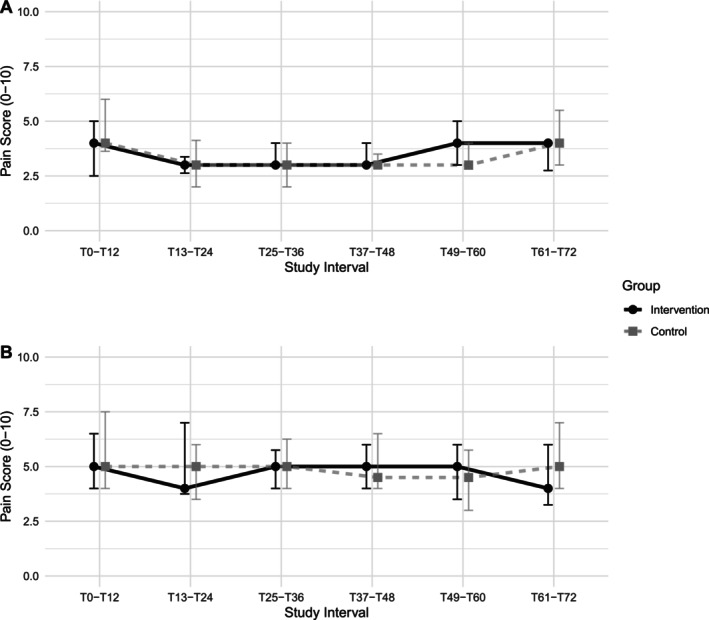
Method: We conducted a double-blinded randomized controlled trial in 10-19 years old, ASA I-III, undergoing single-stage scoliosis correction. Participants were randomly allocated to the Intervention group (intravenous lidocaine 1 mg kg-1 bolus at anesthesia start, followed by 2 mg kg-1 h-1 infusion for 8 h, followed by 1 mg kg-1 h-1 for 40 h) or Control (normal saline). Participants received standardized perioperative multimodal analgesia, including a postoperative morphine infusion with titration rules protocolized to self-reported pain scores. The primary outcome was 48-h morphine utilization; secondary outcomes were median and worst pain scores, and times to first stand, first walk > 15 steps, urinary catheter removal, termination of morphine infusion, and hospital discharge.
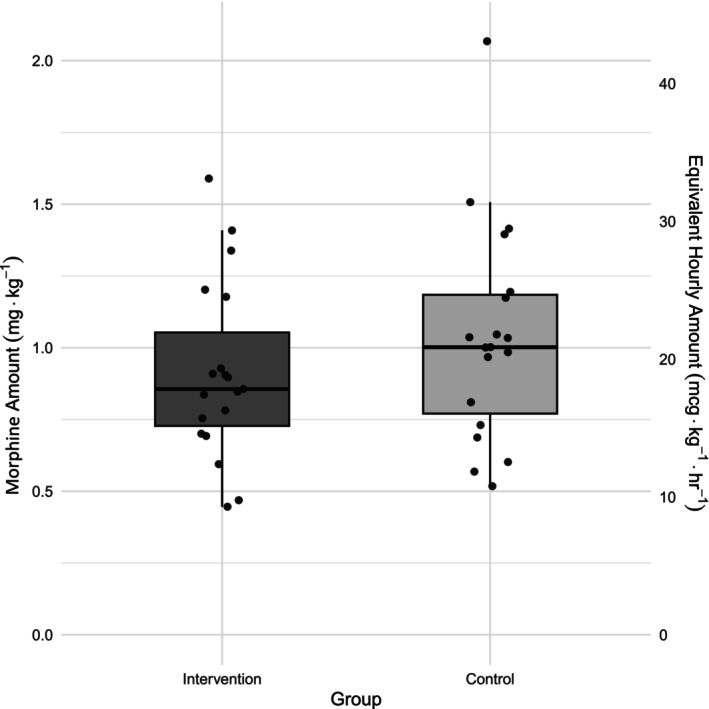
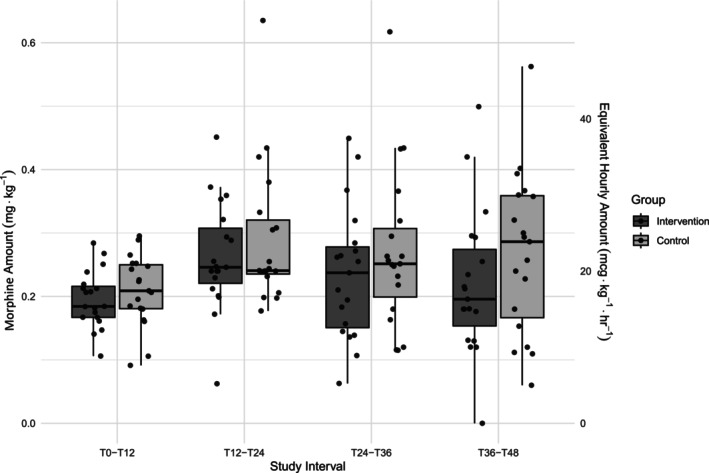
Results: Data were available from 38 participants: 32 (84%) female; median (IQR) age 16.3 (14.9-17.2) years, with curve magnitude (Cobb angle) 62 (56-70) degrees. The 48-h morphine utilization did not differ between groups: Intervention median (IQR) 0.86 (0.73-1.05) mg kg-1 versus Control 1.00 (0.77-1.18) mg kg-1; median difference -0.11 (95% CI -0.30 to 0.13) mg kg-1; p = 0.264. There were similarly no differences in morphine utilization at 12, 24, or 36 h or any secondary outcome, except the first postoperative pain score: Intervention 3/10 (1.75-5) versus Control 5/10 (3-7); median difference -2 (95% CI 0 to -3); p = 0.035. Three cases with mild symptoms of suspected local anesthetic systemic toxicity were observed in the Intervention group.
Conclusions: We found no evidence to support the adjunctive use of 48-h perioperative intravenous lidocaine therapy in adolescents undergoing scoliosis correction in which effective multimodal analgesia was adopted.
期刊介绍:
Devoted to the dissemination of research of interest and importance to practising anesthetists everywhere, the scientific and clinical content of Pediatric Anesthesia covers a wide selection of medical disciplines in all areas relevant to paediatric anaesthesia, pain management and peri-operative medicine. The International Editorial Board is supported by the Editorial Advisory Board and a team of Senior Advisors, to ensure that the journal is publishing the best work from the front line of research in the field. The journal publishes high-quality, relevant scientific and clinical research papers, reviews, commentaries, pro-con debates, historical vignettes, correspondence, case presentations and book reviews.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


