Jerzy Jaskuła, Goran Medic, Sanjay Verma, Joachim Maurer, Tom A Kooy, Bianca de Greef
{"title":"Cost-Effectiveness of a Community First Responder System for Out-of-Hospital Cardiac Arrest in Poland.","authors":"Jerzy Jaskuła, Goran Medic, Sanjay Verma, Joachim Maurer, Tom A Kooy, Bianca de Greef","doi":"10.2147/CEOR.S510907","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Out-of-Hospital Cardiac Arrest (OHCA) is a significant public health issue in Poland, with only an 8.4% survival rate to hospital discharge. Early initiation of Basic Life Support and defibrillation through a Community First Responder (CFR) system can markedly improve survival rates and neurological outcomes.</p><p><strong>Methods: </strong>A decision tree and Markov model compared the cost-effectiveness of three scenarios against standard care by estimating costs and quality-adjusted life years (QALYs). Scenario 1 involved raising public awareness and educating on the 30:2 CPR protocol. Scenario 2 added equipping blue-light service vehicles with Automated External Defibrillators (AEDs) and training personnel. Scenario 3 implemented a full CFR system with integrated AEDs, dispatch centers, and trained citizen responders. The analysis included survival to hospital discharge, with sensitivity analyses assessing robustness.</p><p><strong>Results: </strong>The incremental cost-effectiveness ratios (ICERs) were €15,221 for Scenario 1, €30,659 for Scenario 2, and €16,205 for Scenario 3 per QALY gained-all below the threshold of €50,197. Improvements were observed in all stages, including survival to hospital discharge and neurologically intact survival. Probabilistic sensitivity analyses confirmed the robustness of the results.</p><p><strong>Conclusion: </strong>Implementing a CFR system in Poland is a cost-effective strategy that enhances survival rates after OHCA at an acceptable cost per QALY. The study emphasizes the importance of AED accessibility, trained CFRs, and streamlined emergency responses to improve survival and quality of life for OHCA patients. These findings support policy development and resource allocation to strengthen Poland's emergency medical response to OHCA.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"375-386"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12054549/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S510907","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Out-of-Hospital Cardiac Arrest (OHCA) is a significant public health issue in Poland, with only an 8.4% survival rate to hospital discharge. Early initiation of Basic Life Support and defibrillation through a Community First Responder (CFR) system can markedly improve survival rates and neurological outcomes.
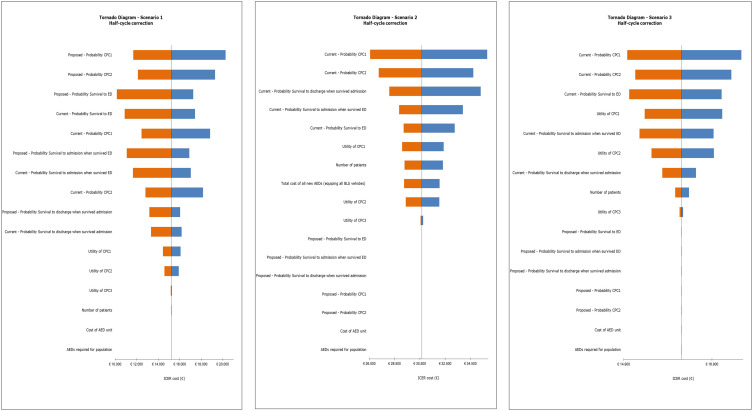
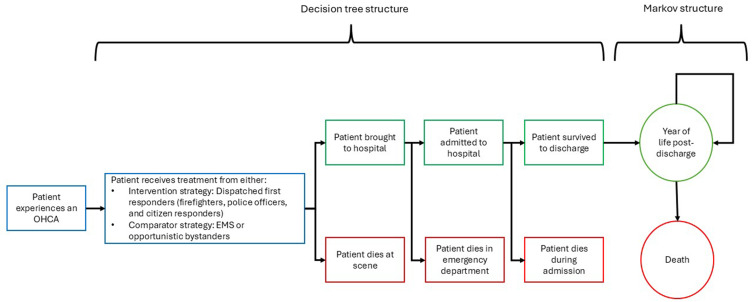
Methods: A decision tree and Markov model compared the cost-effectiveness of three scenarios against standard care by estimating costs and quality-adjusted life years (QALYs). Scenario 1 involved raising public awareness and educating on the 30:2 CPR protocol. Scenario 2 added equipping blue-light service vehicles with Automated External Defibrillators (AEDs) and training personnel. Scenario 3 implemented a full CFR system with integrated AEDs, dispatch centers, and trained citizen responders. The analysis included survival to hospital discharge, with sensitivity analyses assessing robustness.
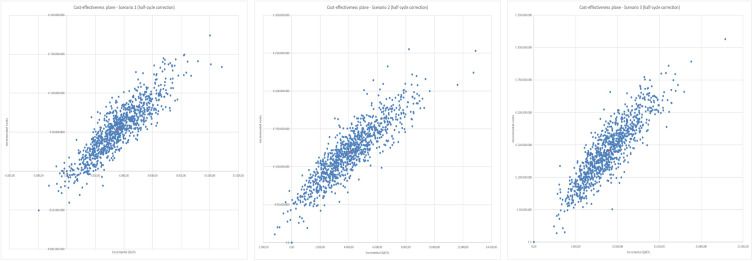
Results: The incremental cost-effectiveness ratios (ICERs) were €15,221 for Scenario 1, €30,659 for Scenario 2, and €16,205 for Scenario 3 per QALY gained-all below the threshold of €50,197. Improvements were observed in all stages, including survival to hospital discharge and neurologically intact survival. Probabilistic sensitivity analyses confirmed the robustness of the results.
Conclusion: Implementing a CFR system in Poland is a cost-effective strategy that enhances survival rates after OHCA at an acceptable cost per QALY. The study emphasizes the importance of AED accessibility, trained CFRs, and streamlined emergency responses to improve survival and quality of life for OHCA patients. These findings support policy development and resource allocation to strengthen Poland's emergency medical response to OHCA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


