Impacts of Premature Atrial Contractions and Biochemical Markers Early After Cryoballoon Versus Radiofrequency Ablation on the Late Recurrence of Atrial Fibrillation.
{"title":"Impacts of Premature Atrial Contractions and Biochemical Markers Early After Cryoballoon Versus Radiofrequency Ablation on the Late Recurrence of Atrial Fibrillation.","authors":"Kenichi Sasaki, Daisuke Togashi, Akira Kasagawa, Ikutaro Nakajima, Takumi Higuma, Tomoo Harada, Yoshihiro J Akashi","doi":"10.19102/icrm.2025.16043","DOIUrl":null,"url":null,"abstract":"<p><p>We sought to clarify the impacts of premature atrial contractions (PACs) and biochemical markers early after cryoballoon (CB) versus radiofrequency (RF) ablation for atrial fibrillation (AF) on the late recurrence of AF (LRAF). The study population included 138 patients who underwent first-time ablation for paroxysmal AF with CB (<i>n</i> = 69) or RF (<i>n</i> = 69). We compared the levels of the PAC burden on Holter monitoring, myocardial-bound creatine kinase (CK-MB), troponin T (TnT), and C-reactive protein (CRP) the day after ablation, and we assessed the incidence of LRAF, which was defined as AF after a 3-month blanking period. The postprocedural PAC burden was not significantly different between the CB and RF groups (<i>P</i> = .35), whereas the CK-MB and CRP levels were significantly higher in the CB group (both <i>P</i> < .01); the TnT levels of the groups were similar (<i>P</i> = .63). Among these, only a higher PAC burden was significantly associated with LRAF in both the CB (top quartile [≥2.16%]: 58% vs. others: 17%; log-rank <i>P</i> = .01) and RF (top quartile [≥3.05%]: 36% vs. others: 9%; log-rank <i>P</i> < .01) groups. A Cox regression analysis revealed two significant predictors of LRAF: in-hospital recurrence (CB group: hazard ratio [HR], 3.55 [1.67-11.80]; <i>P</i> = .04; RF group: HR, 7.55 [1.67-34.20]; <i>P</i> = .01) and a higher postprocedural PAC burden (CB: HR, 1.54 [1.06-2.22]; <i>P</i> = .02; RF: HR, 1.90 [1.16-3.35]; <i>P</i> = .01). In conclusion, irrespective of the ablation modality, the next-day PAC burden (but not the biochemical markers examined herein) is useful for predicting LRAF. Early AF recurrence should be considered a future risk even at the beginning of the blanking period.</p>","PeriodicalId":36299,"journal":{"name":"Journal of Innovations in Cardiac Rhythm Management","volume":"16 4","pages":"6251-6259"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12002004/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innovations in Cardiac Rhythm Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19102/icrm.2025.16043","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
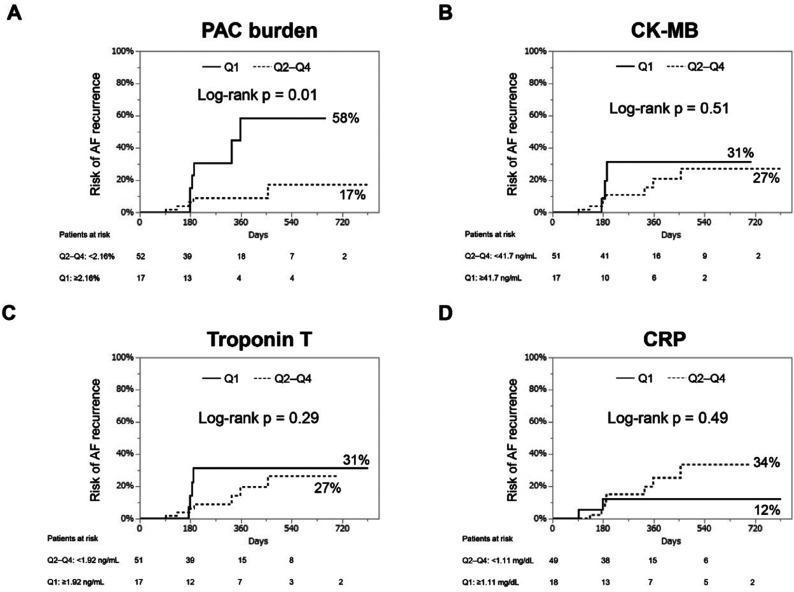
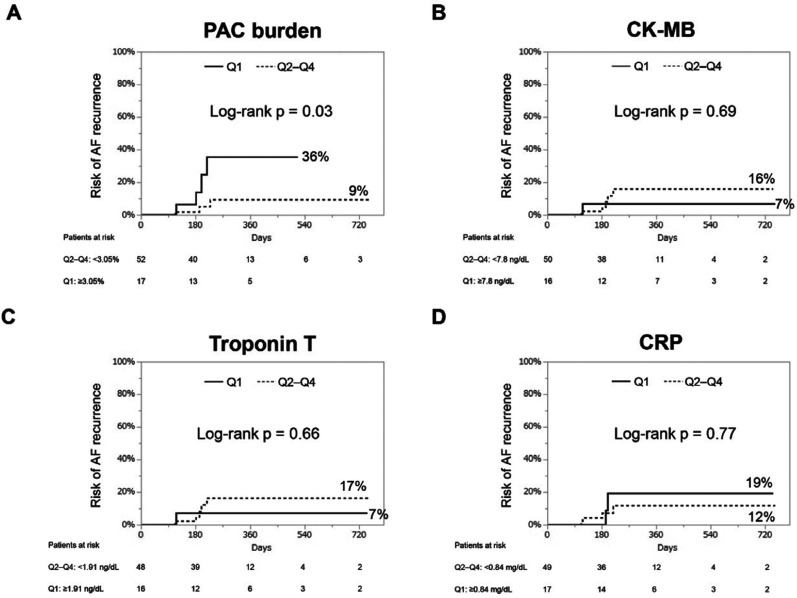
We sought to clarify the impacts of premature atrial contractions (PACs) and biochemical markers early after cryoballoon (CB) versus radiofrequency (RF) ablation for atrial fibrillation (AF) on the late recurrence of AF (LRAF). The study population included 138 patients who underwent first-time ablation for paroxysmal AF with CB (n = 69) or RF (n = 69). We compared the levels of the PAC burden on Holter monitoring, myocardial-bound creatine kinase (CK-MB), troponin T (TnT), and C-reactive protein (CRP) the day after ablation, and we assessed the incidence of LRAF, which was defined as AF after a 3-month blanking period. The postprocedural PAC burden was not significantly different between the CB and RF groups (P = .35), whereas the CK-MB and CRP levels were significantly higher in the CB group (both P < .01); the TnT levels of the groups were similar (P = .63). Among these, only a higher PAC burden was significantly associated with LRAF in both the CB (top quartile [≥2.16%]: 58% vs. others: 17%; log-rank P = .01) and RF (top quartile [≥3.05%]: 36% vs. others: 9%; log-rank P < .01) groups. A Cox regression analysis revealed two significant predictors of LRAF: in-hospital recurrence (CB group: hazard ratio [HR], 3.55 [1.67-11.80]; P = .04; RF group: HR, 7.55 [1.67-34.20]; P = .01) and a higher postprocedural PAC burden (CB: HR, 1.54 [1.06-2.22]; P = .02; RF: HR, 1.90 [1.16-3.35]; P = .01). In conclusion, irrespective of the ablation modality, the next-day PAC burden (but not the biochemical markers examined herein) is useful for predicting LRAF. Early AF recurrence should be considered a future risk even at the beginning of the blanking period.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


