Risk factors influencing periprosthetic fracture and mortality following total hip arthroplasty with a cemented, collarless, polished taper femoral component : a minimum ten-year follow-up cohort study.
Bin Chen, Nick D Clement, Gareth S Turnbull, Chloe E H Scott, Paul Gaston, Gavin J Macpherson, James T Patton
{"title":"Risk factors influencing periprosthetic fracture and mortality following total hip arthroplasty with a cemented, collarless, polished taper femoral component : a minimum ten-year follow-up cohort study.","authors":"Bin Chen, Nick D Clement, Gareth S Turnbull, Chloe E H Scott, Paul Gaston, Gavin J Macpherson, James T Patton","doi":"10.1302/2633-1462.65.BJO-2025-0008.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The aims of this study were to evaluate the incidence of reoperation (all-cause and specifically for periprosthetic femoral fracture (PFF)) and mortality, and associated risk factors, following total hip arthroplasty (THA) incorporating a cemented collarless polished taper slip (PTS) femoral component.</p><p><strong>Methods: </strong>This study included a consecutive series of THAs performed with an Exeter PTS between January 2011 and December 2013 at a single centre. Patient demographics, diabetes, American Society of Anesthesiologists (ASA) grade, and admission type were collected. Co-primary outcomes were reoperation and death.</p><p><strong>Results: </strong>The cohort consisted of 2,177 patients (mean age 66.9 years (SD 11.8)). The median follow-up was 11 years (IQR 10.5 to 11.8). The indications for reoperation were PFF (n = 35, 1.6%), dislocation (n = 15, 0.7%), aseptic cup loosening (n = 13, 0.6%), and infection (n = 10, 0.5%). No femoral components were revised for aseptic loosening. The ten-year aseptic survival for the femoral components was 96.5% (95% CI 95.3 to 97.7). ASA grade III to IV was associated with a higher risk of both all-cause reoperation (hazard ratio (HR) 1.86, p = 0.017) and aseptic reoperation (HR 1.82, p = 0.031). The ten-year PFF-related femoral component survival was 97.7% (95% CI 96.9 to 98.5) and older age (HR 1.05, p = 0.004) and diabetes (HR 2.32, p = 0.048) were independently associated with the occurrence of PFF. Overall patient survival at ten years was 66.1% (95% CI 63.4 to 68.8), with male sex (HR 1.23, p = 0.010), older age (HR 1.08, p < 0.001), ASA grade II to IV (HR 2.22, 4.14 and 6.74, respectively, p ≤ 0.001), and THA undertaken for trauma (HR 1.79, p < 0.001) being independently associated with an increased mortality risk.</p><p><strong>Conclusion: </strong>The cemented PTS demonstrated excellent long-term survival in THA, but PFF was the most common reason for reoperation. Older age and diabetes were independently associated with PFFs. Higher ASA grade was linked to increased risk of both all-cause and aseptic reoperations. Mortality at ten years was influenced by male sex, older age, higher ASA grade, and trauma-related THA.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 5","pages":"544-552"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12052418/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.65.BJO-2025-0008.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: The aims of this study were to evaluate the incidence of reoperation (all-cause and specifically for periprosthetic femoral fracture (PFF)) and mortality, and associated risk factors, following total hip arthroplasty (THA) incorporating a cemented collarless polished taper slip (PTS) femoral component.
Methods: This study included a consecutive series of THAs performed with an Exeter PTS between January 2011 and December 2013 at a single centre. Patient demographics, diabetes, American Society of Anesthesiologists (ASA) grade, and admission type were collected. Co-primary outcomes were reoperation and death.
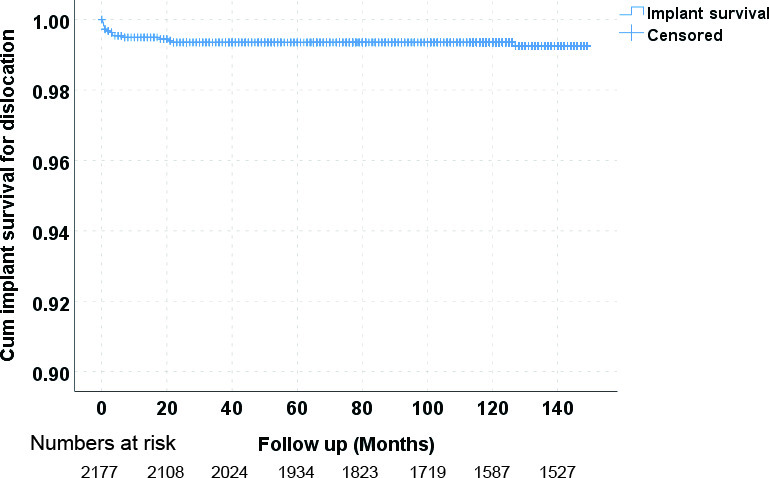
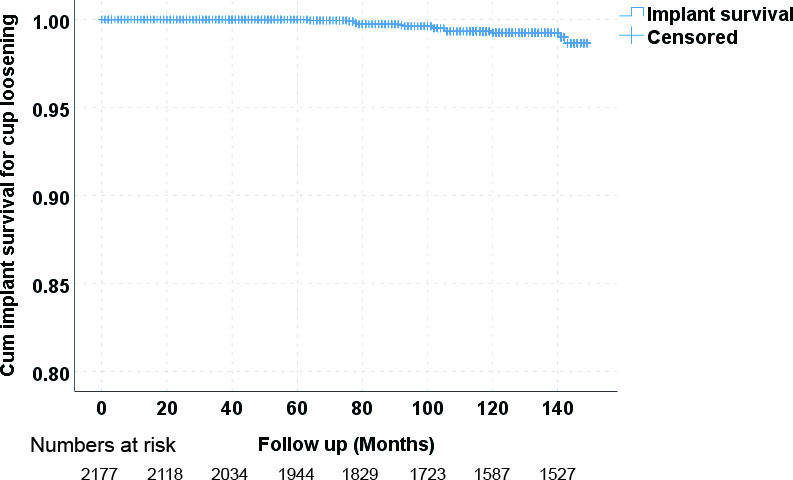
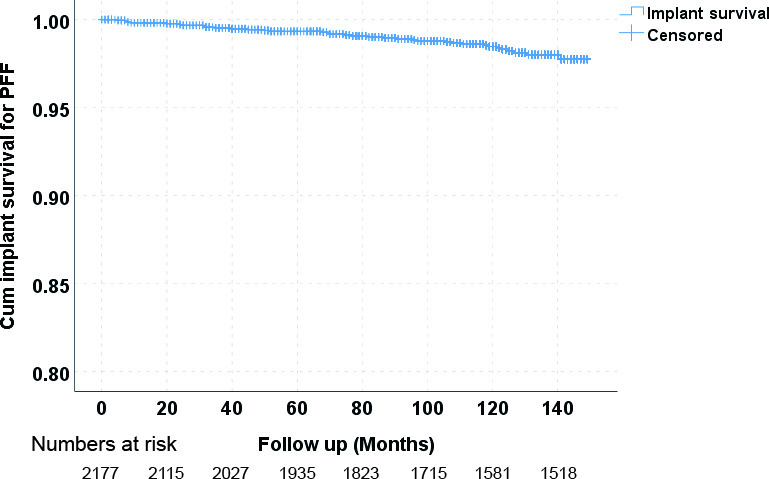
Results: The cohort consisted of 2,177 patients (mean age 66.9 years (SD 11.8)). The median follow-up was 11 years (IQR 10.5 to 11.8). The indications for reoperation were PFF (n = 35, 1.6%), dislocation (n = 15, 0.7%), aseptic cup loosening (n = 13, 0.6%), and infection (n = 10, 0.5%). No femoral components were revised for aseptic loosening. The ten-year aseptic survival for the femoral components was 96.5% (95% CI 95.3 to 97.7). ASA grade III to IV was associated with a higher risk of both all-cause reoperation (hazard ratio (HR) 1.86, p = 0.017) and aseptic reoperation (HR 1.82, p = 0.031). The ten-year PFF-related femoral component survival was 97.7% (95% CI 96.9 to 98.5) and older age (HR 1.05, p = 0.004) and diabetes (HR 2.32, p = 0.048) were independently associated with the occurrence of PFF. Overall patient survival at ten years was 66.1% (95% CI 63.4 to 68.8), with male sex (HR 1.23, p = 0.010), older age (HR 1.08, p < 0.001), ASA grade II to IV (HR 2.22, 4.14 and 6.74, respectively, p ≤ 0.001), and THA undertaken for trauma (HR 1.79, p < 0.001) being independently associated with an increased mortality risk.
Conclusion: The cemented PTS demonstrated excellent long-term survival in THA, but PFF was the most common reason for reoperation. Older age and diabetes were independently associated with PFFs. Higher ASA grade was linked to increased risk of both all-cause and aseptic reoperations. Mortality at ten years was influenced by male sex, older age, higher ASA grade, and trauma-related THA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


