Preoperative and Postoperative Residual Urine in 796 Men Older than 65 Years Undergoing Elective Orthopaedic Surgery in Denmark: A Single-Center Cohort Study.
Inger Markussen Gryet, Charlotte Graugaard-Jensen, Asger Roer Pedersen, Simon Toftgaard Skov
{"title":"Preoperative and Postoperative Residual Urine in 796 Men Older than 65 Years Undergoing Elective Orthopaedic Surgery in Denmark: A Single-Center Cohort Study.","authors":"Inger Markussen Gryet, Charlotte Graugaard-Jensen, Asger Roer Pedersen, Simon Toftgaard Skov","doi":"10.2106/JBJS.OA.24.00180","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postvoid residual urine (PVR) can be an unknown chronic disorder, or it can occur after surgery. A pilot study led to development of a flowchart suggesting performing preoperative and postoperative bladder scans and recommending men with PVR further diagnostic work-up. This study aimed to determine the prevalence of preoperative and postoperative PVR in men older than 65 years undergoing major elective orthopaedic surgery and also to determine risk factors and possibility of prediction.</p><p><strong>Methods: </strong>This was a single-center cohort study. The patients were consecutively included for 1 year from April 2022. Data were extracted from the electronic patient files: age, lower urinary tract symptoms (LUTS), comorbidity, type of surgery and anesthesia, opioid use, and preoperative and postoperative PVR which was defined as ≥150 ml.</p><p><strong>Results: </strong>A total of 796 men were eligible for inclusion: 316 knee, 276 hip, and 26 shoulder arthroplasties and 178 lower back spinal surgeries. Preoperative bladder scans were acquired in 95% of the eligible patients, and PVR was found in 15% (confidence interval [CI] 12-18). There was a higher risk of preoperative PVR in men reporting LUTS, OR 1.97 (1.28-3.03); neurological disease, OR 3.09 (1.41-6.74); and the risk increased with higher age, OR 1.08 per year (1.04-1.12). PVR was found in 9% of the men without risk factors. A postoperative bladder scan was performed in 72% of the men. Among men without preoperative PVR, 15% (CI 12-19) had postoperative PVR de novo. The highest risk for PVR postoperative was PVR preoperatively.</p><p><strong>Conclusions: </strong>Preoperatively, 15% had PVR. Neurological disease, LUTS, and higher age were identified as risk factors, but PVR was found in 9% of the men without risk factors. In men without preoperative PVR, 15% had postoperative PVR de novo. It is not possible to conclude whether PVR is transient or chronic, and it is unclear whether a PVR of 150 ml is associated with complications or if the threshold should be higher. This study highlights the importance of awareness regarding voiding issues before and after surgery.</p><p><strong>Level of evidence: </strong>Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 2","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12040042/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.24.00180","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
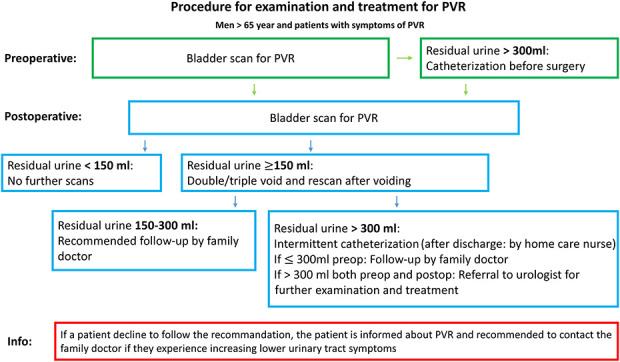
Background: Postvoid residual urine (PVR) can be an unknown chronic disorder, or it can occur after surgery. A pilot study led to development of a flowchart suggesting performing preoperative and postoperative bladder scans and recommending men with PVR further diagnostic work-up. This study aimed to determine the prevalence of preoperative and postoperative PVR in men older than 65 years undergoing major elective orthopaedic surgery and also to determine risk factors and possibility of prediction.
Methods: This was a single-center cohort study. The patients were consecutively included for 1 year from April 2022. Data were extracted from the electronic patient files: age, lower urinary tract symptoms (LUTS), comorbidity, type of surgery and anesthesia, opioid use, and preoperative and postoperative PVR which was defined as ≥150 ml.
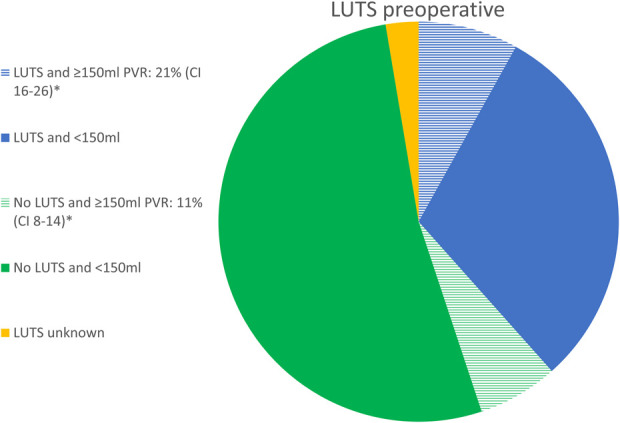
Results: A total of 796 men were eligible for inclusion: 316 knee, 276 hip, and 26 shoulder arthroplasties and 178 lower back spinal surgeries. Preoperative bladder scans were acquired in 95% of the eligible patients, and PVR was found in 15% (confidence interval [CI] 12-18). There was a higher risk of preoperative PVR in men reporting LUTS, OR 1.97 (1.28-3.03); neurological disease, OR 3.09 (1.41-6.74); and the risk increased with higher age, OR 1.08 per year (1.04-1.12). PVR was found in 9% of the men without risk factors. A postoperative bladder scan was performed in 72% of the men. Among men without preoperative PVR, 15% (CI 12-19) had postoperative PVR de novo. The highest risk for PVR postoperative was PVR preoperatively.
Conclusions: Preoperatively, 15% had PVR. Neurological disease, LUTS, and higher age were identified as risk factors, but PVR was found in 9% of the men without risk factors. In men without preoperative PVR, 15% had postoperative PVR de novo. It is not possible to conclude whether PVR is transient or chronic, and it is unclear whether a PVR of 150 ml is associated with complications or if the threshold should be higher. This study highlights the importance of awareness regarding voiding issues before and after surgery.
Level of evidence: Level III. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


