Eleni Domzaridou, Matthew J Carr, David M Williams, Anthony J Avery, Tjeerd van Staa, D Aled Rees, Darren M Ashcroft
{"title":"Treatment Persistence and Variations in Prescribing Oral, Injectable, and Inhaled Corticosteroids: A Population-Based Drug Utilisation Study.","authors":"Eleni Domzaridou, Matthew J Carr, David M Williams, Anthony J Avery, Tjeerd van Staa, D Aled Rees, Darren M Ashcroft","doi":"10.1002/pds.70153","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To examine variation in oral, injectable, and inhaled corticosteroid (CS) prescribing in primary care, exploring treatment persistence and coverage.</p><p><strong>Methods: </strong>We examined patient-level electronic health records from English general practices in the Clinical Practice Research Datalink Aurum database. We delineated a cohort of new users of oral, injectable, or inhaled CS with prescriptions issued between January 1, 2000, and June 30, 2021. Lorenz curves assessed potential prescribing skewness, and Kaplan-Meier (KM) plots estimated treatment persistence. The Proportion of Patients Covered (PPC) method estimated the proportion of patients still covered by treatment 1 year after initiation.</p><p><strong>Results: </strong>We observed 1 942 571 CS users across 1471 general practices, with 20% of oral and inhaled CS users accounting for almost 80% of total CS use. Older patients with comorbidities including respiratory diseases (13.5%), skin conditions (5.8%), or inflammatory bowel diseases (1.6%) were more likely to be prescribed higher doses. The KM plots showed that 20% of oral and 50% of inhaled CS users were persistent after one and 2 months, respectively. The PPC method indicated that 30% of oral and 60% of inhaled CS users were covered by treatment 6 months post-initiation. Some variation was observed when different grace periods were applied. Combined use of oral and inhaled CS was observed for 6.9% of patients.</p><p><strong>Conclusion: </strong>A fifth of patients receiving CS accounted for over 80% of oral and inhaled CS prescribing in primary care. Identifying these patients is crucial for targeting future interventions to promote patient safety and cost-effective CS use.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 5","pages":"e70153"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12042156/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70153","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To examine variation in oral, injectable, and inhaled corticosteroid (CS) prescribing in primary care, exploring treatment persistence and coverage.
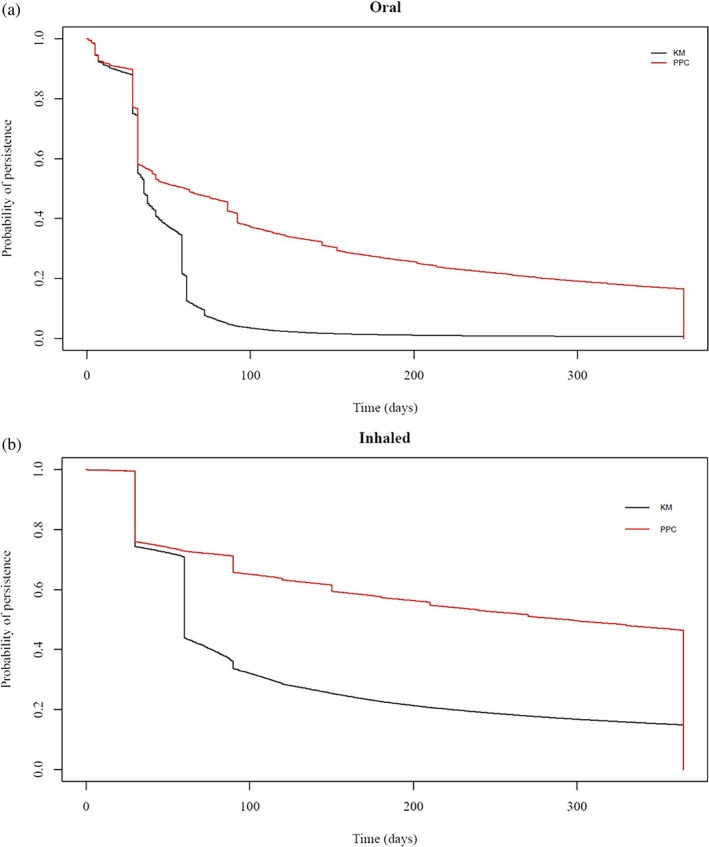
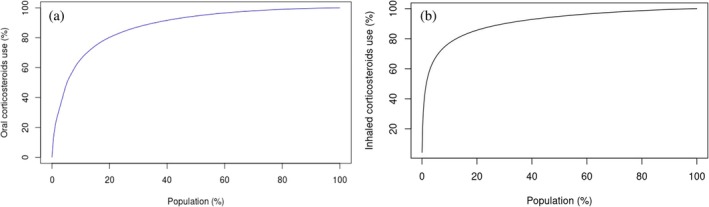
Methods: We examined patient-level electronic health records from English general practices in the Clinical Practice Research Datalink Aurum database. We delineated a cohort of new users of oral, injectable, or inhaled CS with prescriptions issued between January 1, 2000, and June 30, 2021. Lorenz curves assessed potential prescribing skewness, and Kaplan-Meier (KM) plots estimated treatment persistence. The Proportion of Patients Covered (PPC) method estimated the proportion of patients still covered by treatment 1 year after initiation.
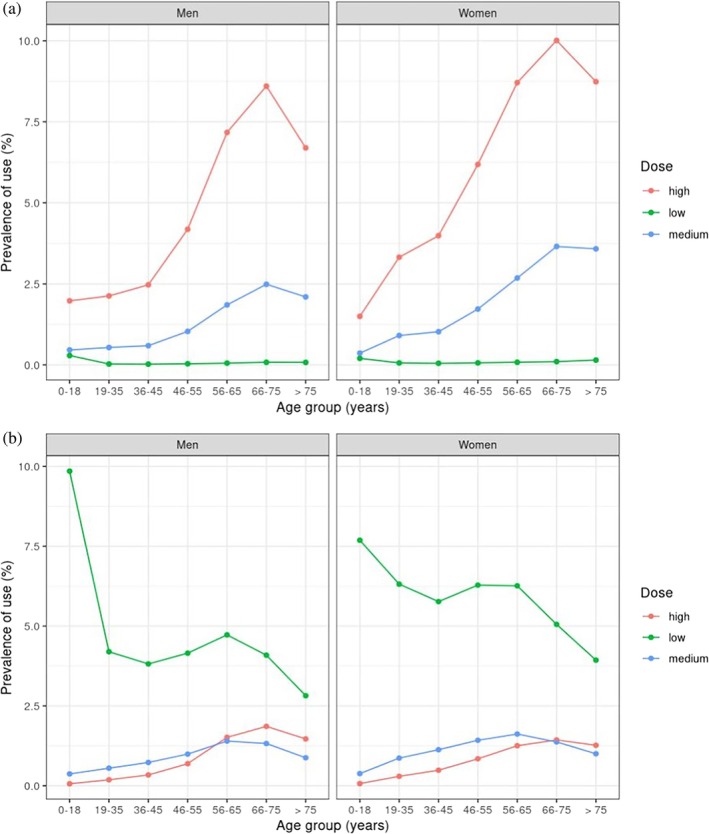
Results: We observed 1 942 571 CS users across 1471 general practices, with 20% of oral and inhaled CS users accounting for almost 80% of total CS use. Older patients with comorbidities including respiratory diseases (13.5%), skin conditions (5.8%), or inflammatory bowel diseases (1.6%) were more likely to be prescribed higher doses. The KM plots showed that 20% of oral and 50% of inhaled CS users were persistent after one and 2 months, respectively. The PPC method indicated that 30% of oral and 60% of inhaled CS users were covered by treatment 6 months post-initiation. Some variation was observed when different grace periods were applied. Combined use of oral and inhaled CS was observed for 6.9% of patients.
Conclusion: A fifth of patients receiving CS accounted for over 80% of oral and inhaled CS prescribing in primary care. Identifying these patients is crucial for targeting future interventions to promote patient safety and cost-effective CS use.
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


