Giancarlo Pesce, Mit Patel, Gaelle Gusto, Ananth Kadambi, Aastha Chandak, Terri Madison
{"title":"Real-world challenges associated with the use of four common systemic glucocorticoids in a United States IgAN cohort.","authors":"Giancarlo Pesce, Mit Patel, Gaelle Gusto, Ananth Kadambi, Aastha Chandak, Terri Madison","doi":"10.3389/fneph.2025.1574239","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To understand the difference in adverse events (AEs), healthcare resource utilization (HCRU), and kidney failure rates in immunoglobulin A nephropathy (IgAN) patients who initiated systemic glucocorticoid (SGC) treatment compared with those who did not.</p><p><strong>Methods: </strong>The overall cohort was selected from patients with IgAN (ICD-10 codes N02.8 and N04.1) identified in the TriNetX Dataworks database between January 2011 and May 2022. New initiators of dexamethasone, prednisone, prednisolone, or methylprednisolone (SGC cohort) were propensity score (PS) matched 1:1 with patients who did not receive SGC (non-SGC cohort) based on their characteristics at diagnosis. The index date was the date of SGC initiation; for the non-SGC cohort, a pseudo-index date was assigned using the same lag from diagnosis to index date as their PS-matched pairs. Patients with kidney failure before the index/pseudo-index date and their 1:1 PS-matched pairs were excluded.</p><p><strong>Results: </strong>The final analysis was conducted in 802 patients (401 PS-matched pairs, mean age 41.2 years, 55% male). Median duration of follow-up was 3.5 and 3.1 years for the SGC and non-SGC cohorts, respectively. Compared with the non-SGC cohort, patients in the SGC cohort had greater frequency of several AEs, including severe infections, greater annualized HCRU and costs, and greater incidence of kidney failure.</p><p><strong>Conclusions: </strong>This study found that SGC therapy may increase adverse reactions and HCRU in IgAN patients, while comparatively providing no beneficial effects on preserving kidney function.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"5 ","pages":"1574239"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12058894/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2025.1574239","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To understand the difference in adverse events (AEs), healthcare resource utilization (HCRU), and kidney failure rates in immunoglobulin A nephropathy (IgAN) patients who initiated systemic glucocorticoid (SGC) treatment compared with those who did not.
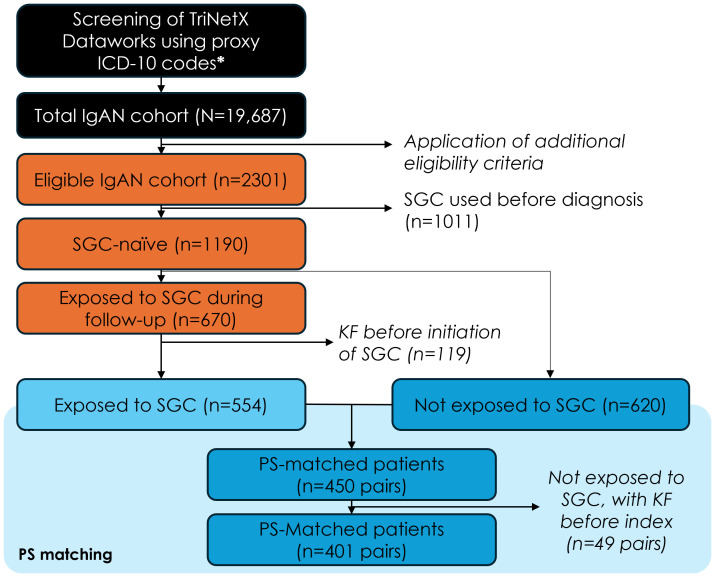
Methods: The overall cohort was selected from patients with IgAN (ICD-10 codes N02.8 and N04.1) identified in the TriNetX Dataworks database between January 2011 and May 2022. New initiators of dexamethasone, prednisone, prednisolone, or methylprednisolone (SGC cohort) were propensity score (PS) matched 1:1 with patients who did not receive SGC (non-SGC cohort) based on their characteristics at diagnosis. The index date was the date of SGC initiation; for the non-SGC cohort, a pseudo-index date was assigned using the same lag from diagnosis to index date as their PS-matched pairs. Patients with kidney failure before the index/pseudo-index date and their 1:1 PS-matched pairs were excluded.
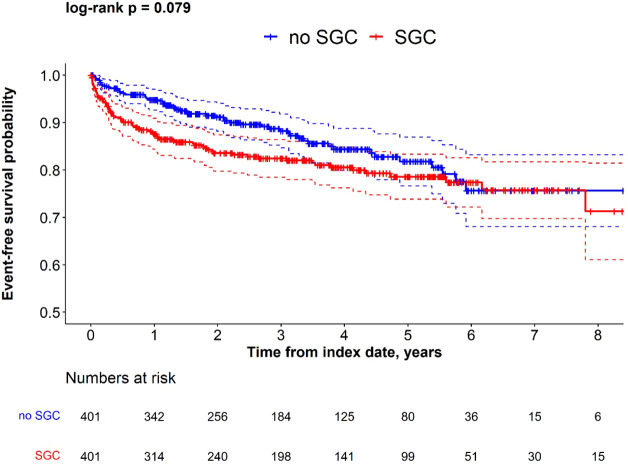
Results: The final analysis was conducted in 802 patients (401 PS-matched pairs, mean age 41.2 years, 55% male). Median duration of follow-up was 3.5 and 3.1 years for the SGC and non-SGC cohorts, respectively. Compared with the non-SGC cohort, patients in the SGC cohort had greater frequency of several AEs, including severe infections, greater annualized HCRU and costs, and greater incidence of kidney failure.
Conclusions: This study found that SGC therapy may increase adverse reactions and HCRU in IgAN patients, while comparatively providing no beneficial effects on preserving kidney function.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


