The association between urgency level and hospital admission, mortality and resource utilization in three emergency department triage systems: an observational multicenter study.
Marit E van Wegen, Laura F C Fransen, Wendy A M H Thijssen, Georgios Alexandridis, Bas de Groot
{"title":"The association between urgency level and hospital admission, mortality and resource utilization in three emergency department triage systems: an observational multicenter study.","authors":"Marit E van Wegen, Laura F C Fransen, Wendy A M H Thijssen, Georgios Alexandridis, Bas de Groot","doi":"10.1186/s13049-025-01392-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Effective triage systems are crucial for prioritizing patients based on urgency and optimizing resource utilization. An ideal triage system is expected to have low resource utilization, hospitalization and mortality among patients classified at low urgency levels. Furthermore, it should exhibit an increase in the risk of hospitalization and mortality as urgency levels increase, ensuring the most critically ill patients receive priority care first. However, it is unclear which triage system performs best.</p><p><strong>Objective: </strong>To compare the performance of the Manchester Triage System (MTS), the Emergency Severity Index (ESI), and the Netherlands Triage Standard (NTS) by investigating the association between urgency levels and resource utilization, hospitalization and in-hospital mortality in Emergency Department (ED) patients.</p><p><strong>Methods: </strong>Observational multicenter cohort study using data from the Netherlands Emergency department Evaluation Database, comprising seven representative EDs in six Dutch hospitals. All consecutive ED patients with a registered urgency level were included. Resource utilization, hospitalization and mortality were measured across all urgency levels. In each triage system, multivariable logistic regression was used to assess the association between urgency level and in-hospital mortality and hospitalization, adjusting for age, sex, presenting complaints and hospital type.</p><p><strong>Results: </strong>A total of 696,518 ED visits (MTS 320,406 (46.1%), ESI 214,267 (30.8%), NTS 161,845 (23.3%) patients) were included. Resource utilization was substantially lower in the lowest urgency level of the ESI compared to the MTS and NTS. Hospitalization to a regular ward, cardiac, medium or intensive care unit in the least urgent level was 3.9% in the ESI, considerably lower than in the MTS (23.1%) and NTS (34.3%) (P < 0.05). Mortality in the lowest urgency level of the ESI was 0.8%, while in the MTS and NTS this was 6.3% and 12.4%, respectively (P < 0.05). In the ESI, the risk (Adjusted Odds Ratios) for hospitalization and mortality increased much more with increasing urgency levels compared to the MTS and NTS.</p><p><strong>Conclusion: </strong>This study suggests that the ESI may be more effective in distinguishing between patients with low and high urgency, with a reduced risk of undertriage when compared to the MTS and NTS.</p>","PeriodicalId":49292,"journal":{"name":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","volume":"33 1","pages":"72"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12044865/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma Resuscitation & Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-025-01392-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Effective triage systems are crucial for prioritizing patients based on urgency and optimizing resource utilization. An ideal triage system is expected to have low resource utilization, hospitalization and mortality among patients classified at low urgency levels. Furthermore, it should exhibit an increase in the risk of hospitalization and mortality as urgency levels increase, ensuring the most critically ill patients receive priority care first. However, it is unclear which triage system performs best.
Objective: To compare the performance of the Manchester Triage System (MTS), the Emergency Severity Index (ESI), and the Netherlands Triage Standard (NTS) by investigating the association between urgency levels and resource utilization, hospitalization and in-hospital mortality in Emergency Department (ED) patients.
Methods: Observational multicenter cohort study using data from the Netherlands Emergency department Evaluation Database, comprising seven representative EDs in six Dutch hospitals. All consecutive ED patients with a registered urgency level were included. Resource utilization, hospitalization and mortality were measured across all urgency levels. In each triage system, multivariable logistic regression was used to assess the association between urgency level and in-hospital mortality and hospitalization, adjusting for age, sex, presenting complaints and hospital type.
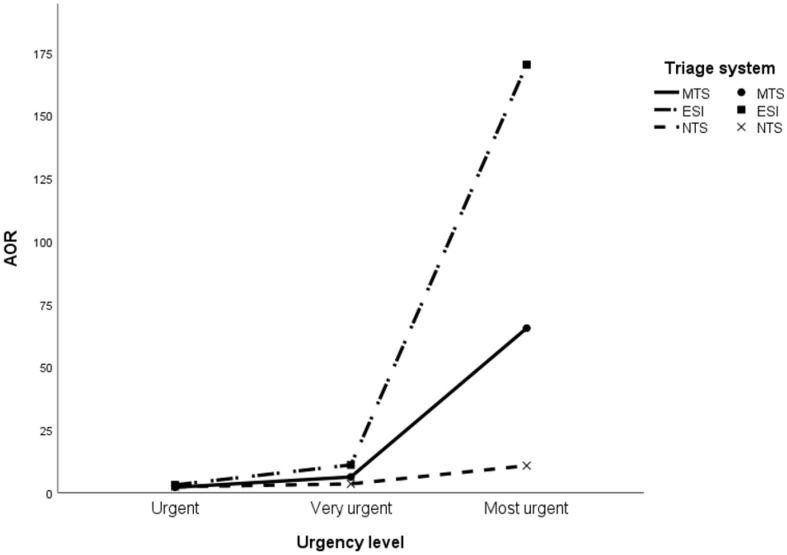
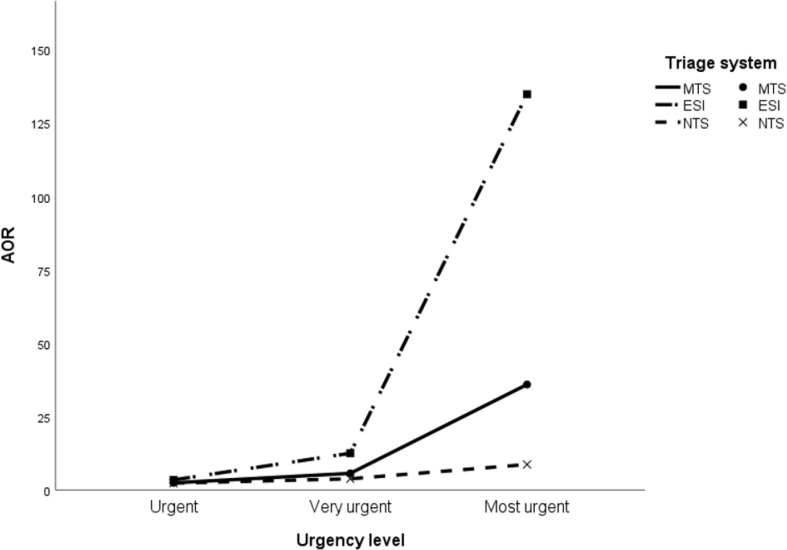
Results: A total of 696,518 ED visits (MTS 320,406 (46.1%), ESI 214,267 (30.8%), NTS 161,845 (23.3%) patients) were included. Resource utilization was substantially lower in the lowest urgency level of the ESI compared to the MTS and NTS. Hospitalization to a regular ward, cardiac, medium or intensive care unit in the least urgent level was 3.9% in the ESI, considerably lower than in the MTS (23.1%) and NTS (34.3%) (P < 0.05). Mortality in the lowest urgency level of the ESI was 0.8%, while in the MTS and NTS this was 6.3% and 12.4%, respectively (P < 0.05). In the ESI, the risk (Adjusted Odds Ratios) for hospitalization and mortality increased much more with increasing urgency levels compared to the MTS and NTS.
Conclusion: This study suggests that the ESI may be more effective in distinguishing between patients with low and high urgency, with a reduced risk of undertriage when compared to the MTS and NTS.
期刊介绍:
The primary topics of interest in Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (SJTREM) are the pre-hospital and early in-hospital diagnostic and therapeutic aspects of emergency medicine, trauma, and resuscitation. Contributions focusing on dispatch, major incidents, etiology, pathophysiology, rehabilitation, epidemiology, prevention, education, training, implementation, work environment, as well as ethical and socio-economic aspects may also be assessed for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


