Sherif Wael, Omar Hamdy, Mohamed Yasser, Sara Elmandrawi, Mai Mostafa, Nouran Mohammed, Ahmed Elghrieb
{"title":"Lytic bone lesion of the skull as a rare manifestation of hepatocellular carcinoma: a case report.","authors":"Sherif Wael, Omar Hamdy, Mohamed Yasser, Sara Elmandrawi, Mai Mostafa, Nouran Mohammed, Ahmed Elghrieb","doi":"10.1186/s13037-025-00434-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatocellular carcinoma (HCC) ranks among the leading causes of cancer-related deaths worldwide, with metastatic spread to bones being alarmingly frequent. However, HCC metastases to the skull are notably rare, accounting for only 0.4-1.6% of all bone metastases. Typically, metastases are found in the spine, pelvis, and ribs. The occurrence of solitary skull metastases, especially in the absence of active primary liver cancer, is extremely uncommon.</p><p><strong>Case description: </strong>We present the clinical case of a 57-year-old male patient with a documented history of hepatitis C virus infection but without prior evidence of active hepatocellular carcinoma. Over the course of several months, he developed a non-tender, progressively enlarging mass located in the occipital region of the skull. A computed tomography (CT) scan identified a lytic lesion with intracranial compression, although no midline shift was noted. Histopathological examination confirmed the lesion as metastatic HCC, further supported by immunohistochemical markers Hepatari- 1 and Cytokeratin- 19. Subsequent diagnostic procedures revealed hepatic lesions, including a positron emission tomography (PET)-CT scan. Further examination through CT imaging of the abdomen with contrast highlighted a well-defined focal lesion in hepatic segment 4a, measuring 4.3 × 4.3 cm, predominantly enhancing with HCC characteristics. The skull lesion was surgically removed en bloc, and the patient underwent adjunct radiotherapy and systemic therapy, with palliative therapy till his death in May 2024. To better understand and manage this atypical presentation, we conducted a review for the discussion of clinical manifestations, imaging findings, pathological features, and patient outcomes associated with HCC skull metastases.</p><p><strong>Conclusion: </strong>This case emphasizes the critical importance of considering hepatocellular carcinoma in the differential diagnosis of solitary skull lesions, especially in patients with risk factors for liver disease. Prompt identification of the primary malignancy remains essential for ensuring optimal management and improving patient prognosis.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"19 1","pages":"12"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12016127/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-025-00434-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hepatocellular carcinoma (HCC) ranks among the leading causes of cancer-related deaths worldwide, with metastatic spread to bones being alarmingly frequent. However, HCC metastases to the skull are notably rare, accounting for only 0.4-1.6% of all bone metastases. Typically, metastases are found in the spine, pelvis, and ribs. The occurrence of solitary skull metastases, especially in the absence of active primary liver cancer, is extremely uncommon.
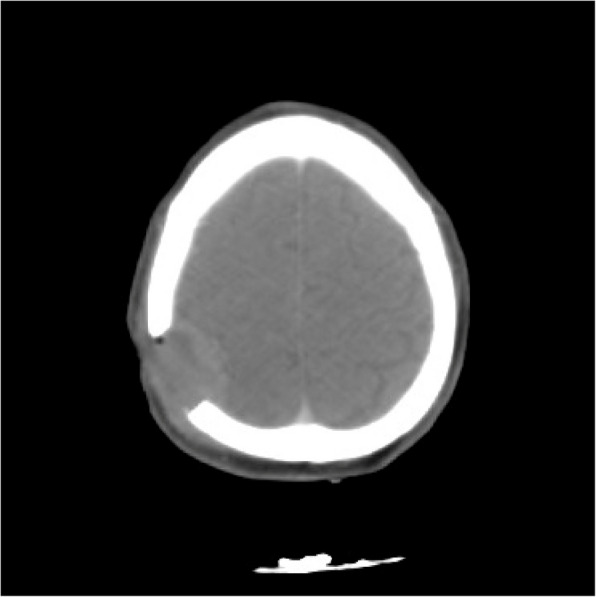
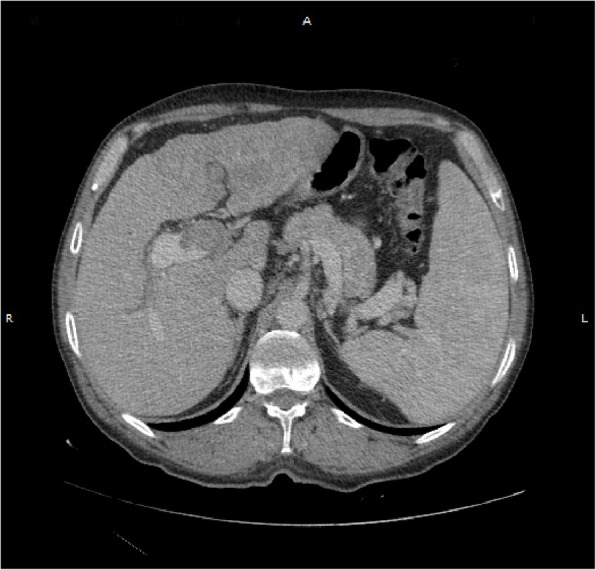
Case description: We present the clinical case of a 57-year-old male patient with a documented history of hepatitis C virus infection but without prior evidence of active hepatocellular carcinoma. Over the course of several months, he developed a non-tender, progressively enlarging mass located in the occipital region of the skull. A computed tomography (CT) scan identified a lytic lesion with intracranial compression, although no midline shift was noted. Histopathological examination confirmed the lesion as metastatic HCC, further supported by immunohistochemical markers Hepatari- 1 and Cytokeratin- 19. Subsequent diagnostic procedures revealed hepatic lesions, including a positron emission tomography (PET)-CT scan. Further examination through CT imaging of the abdomen with contrast highlighted a well-defined focal lesion in hepatic segment 4a, measuring 4.3 × 4.3 cm, predominantly enhancing with HCC characteristics. The skull lesion was surgically removed en bloc, and the patient underwent adjunct radiotherapy and systemic therapy, with palliative therapy till his death in May 2024. To better understand and manage this atypical presentation, we conducted a review for the discussion of clinical manifestations, imaging findings, pathological features, and patient outcomes associated with HCC skull metastases.
Conclusion: This case emphasizes the critical importance of considering hepatocellular carcinoma in the differential diagnosis of solitary skull lesions, especially in patients with risk factors for liver disease. Prompt identification of the primary malignancy remains essential for ensuring optimal management and improving patient prognosis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


