{"title":"High afterload rather than myocardial fibrosis predicts reduced ejection fraction in severe aortic stenosis with afterload mismatch.","authors":"Megan Rian Rajah, Anton Doubell, Philip Herbst","doi":"10.1136/openhrt-2025-003345","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Afterload mismatch (AM) refers to high-gradient (mean gradient ≥40 mm Hg) severe aortic stenosis (AS) with reduced left ventricular ejection fraction (LVEF <50%) that is hypothesised to arise from mechanisms other than true contractile impairment. The extent, pattern and functional impact of myocardial fibrosis (MF), which is associated with systolic impairment, is poorly understood in the context of AM.</p><p><strong>Methods: </strong>High-gradient severe AS patients with (n=25; low ejection fraction high-gradient, LEF-HG) and without (n=33; normal ejection fraction high-gradient (NEF-HG)) reduced LVEF underwent cardiovascular MRI. Using T1 mapping, extracellular volume (ECV) fraction and late gadolinium enhancement (LGE), the extent and pattern of MF was compared between the two groups. End-systolic wall stress (ESWS) as a measure of afterload was estimated, and its relationship with LVEF was compared with that of MF and LVEF.</p><p><strong>Results: </strong>Stenosis severity was worse in the LEF-HG group (aortic valve area 0.5±0.2 vs 0.7±0.2 cm<sup>2</sup>, mean gradient 55 (46-66) vs 48 (41-69) mm Hg). In the LEF-HG group, high ESWS with cavity dilation and significant hypertrophy were observed compared with the NEF-HG group. MF was present in both groups with a significantly higher burden in the LEF-HG group (T1 time 1061±22 vs 1041±33 ms, ECV 26%±3% vs 24%±3%, LGE mass 4.3 (1.7-9.3) vs 0.1 (0.06-3.39) g). The association between MF and LVEF was weak, while ESWS was strongly associated with LVEF (r -0.8, p<0.0001) and was the best predictor of LVEF in multivariate prediction analysis.</p><p><strong>Conclusions: </strong>MF was present in both groups with a higher burden in those with LEF-HG AS. High ESWS, that is, afterload, rather than MF, was the strongest predictor of LVEF. While MF may not directly impact systolic function in AM, it is still an important factor to account for in AS given its association with increased mortality.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 1","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12060870/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003345","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Afterload mismatch (AM) refers to high-gradient (mean gradient ≥40 mm Hg) severe aortic stenosis (AS) with reduced left ventricular ejection fraction (LVEF <50%) that is hypothesised to arise from mechanisms other than true contractile impairment. The extent, pattern and functional impact of myocardial fibrosis (MF), which is associated with systolic impairment, is poorly understood in the context of AM.
Methods: High-gradient severe AS patients with (n=25; low ejection fraction high-gradient, LEF-HG) and without (n=33; normal ejection fraction high-gradient (NEF-HG)) reduced LVEF underwent cardiovascular MRI. Using T1 mapping, extracellular volume (ECV) fraction and late gadolinium enhancement (LGE), the extent and pattern of MF was compared between the two groups. End-systolic wall stress (ESWS) as a measure of afterload was estimated, and its relationship with LVEF was compared with that of MF and LVEF.
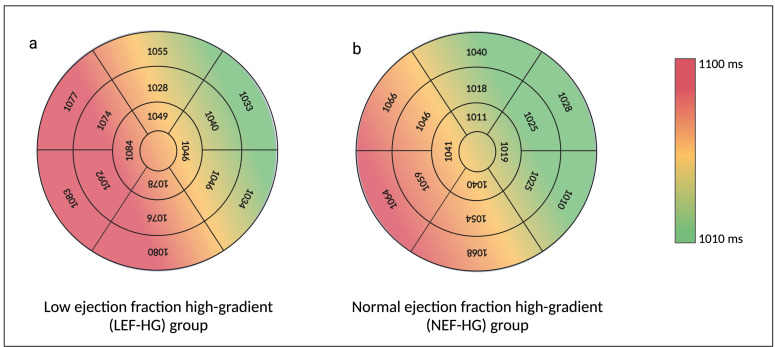
Results: Stenosis severity was worse in the LEF-HG group (aortic valve area 0.5±0.2 vs 0.7±0.2 cm2, mean gradient 55 (46-66) vs 48 (41-69) mm Hg). In the LEF-HG group, high ESWS with cavity dilation and significant hypertrophy were observed compared with the NEF-HG group. MF was present in both groups with a significantly higher burden in the LEF-HG group (T1 time 1061±22 vs 1041±33 ms, ECV 26%±3% vs 24%±3%, LGE mass 4.3 (1.7-9.3) vs 0.1 (0.06-3.39) g). The association between MF and LVEF was weak, while ESWS was strongly associated with LVEF (r -0.8, p<0.0001) and was the best predictor of LVEF in multivariate prediction analysis.
Conclusions: MF was present in both groups with a higher burden in those with LEF-HG AS. High ESWS, that is, afterload, rather than MF, was the strongest predictor of LVEF. While MF may not directly impact systolic function in AM, it is still an important factor to account for in AS given its association with increased mortality.
背景:后负荷不匹配(AM)是指高梯度(平均梯度≥40 mm Hg)严重主动脉瓣狭窄(AS)伴左室射血分数降低(LVEF)。方法:高梯度严重AS患者(n=25;低射血分数高梯度,左旋-汞柱,无(n=33;正常射血分数高梯度(NEF-HG)降低的LVEF行心血管MRI检查。通过T1作图、细胞外体积(ECV)分数和晚期钆增强(LGE),比较两组间MF的范围和模式。估计收缩期末期壁应力(ESWS)作为后负荷的度量,并将其与LVEF的关系与MF和LVEF进行比较。结果:LEF-HG组狭窄程度更严重(主动脉瓣面积0.5±0.2 vs 0.7±0.2 cm2,平均梯度55 (46-66)vs 48 (41-69) mm Hg)。与NEF-HG组相比,左- hg组ESWS高,腔扩张,明显肥厚。两组均存在MF,且LEF-HG组的负担明显更高(T1时间1061±22 ms vs 1041±33 ms, ECV 26%±3% vs 24%±3%,LGE质量4.3 (1.7-9.3)vs 0.1 (0.06-3.39) g)。MF与LVEF的相关性较弱,而ESWS与LVEF的相关性较强(r -0.8)。结论:两组患者均存在MF,且LEF-HG AS患者负担较高。高ESWS,即后负荷,而不是MF,是LVEF的最强预测因子。虽然MF可能不会直接影响AM的收缩功能,但鉴于其与死亡率增加的关联,它仍然是AS的一个重要因素。
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


