Ingrid Engebretsen, Francisco Oteiza, Elisabeth Floberghagen Birkelund, Signe Marie Brandal, Christoffer Bugge, Sigrun Halvorsen
{"title":"Cardiovascular disease in breast cancer patients: a nationwide real-world evidence study 2013-20.","authors":"Ingrid Engebretsen, Francisco Oteiza, Elisabeth Floberghagen Birkelund, Signe Marie Brandal, Christoffer Bugge, Sigrun Halvorsen","doi":"10.1093/ehjopen/oeaf043","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Various measures have been implemented in clinical practice to reduce the risk of cardiovascular complications during breast cancer (BC) treatment. The aim of this study was to investigate whether women diagnosed with BC exhibit a higher incidence of cardiovascular disease (CVD).</p><p><strong>Methods and results: </strong>Matched cohort study. Using data from the Cancer Registry of Norway and the Norwegian Patient Registry, we created a nationwide cohort of women diagnosed with BC between 2013 and 2020 and age-matched controls (matching ratio 1:10). For BC patients, the index date was the date of their BC diagnosis. For controls, the index date was a random date within the index year of the matched BC patient. For eight selected CVDs, we compared the prevalence before BC diagnosis between cases and controls, as well as the overall incidence, hazard ratios (HRs), and cumulative incidences post BC diagnosis. Follow-up was through 2021. Our study population consisted of 27 526 BC patients and 269 904 matched controls. Among the subset of patients without CVD prior to index, BC patients had significantly increased overall and cumulative risk of pulmonary embolism (HR = 3.00, 95% CI: [2.51-3.59]), atrial fibrillation (1.53 [1.38-1.70]), other cardiac arrhythmias (1.43 [1.27-1.61]), heart failure (1.93 [1.33-2.80]), hypertensive heart disease (1.79 [1.67-1.91]), and heart valve disease (2.02 [1.79-2.27]).</p><p><strong>Conclusion: </strong>In this contemporary cohort, BC patients still had an increased risk of several CVDs compared to age-matched controls. Further research is needed to determine the causes of this increased risk, but clinicians should be aware and optimize therapy accordingly.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 3","pages":"oeaf043"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12042752/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf043","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
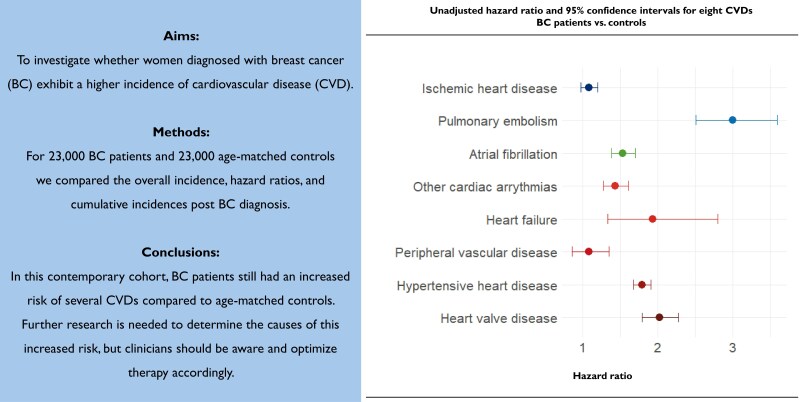
Aims: Various measures have been implemented in clinical practice to reduce the risk of cardiovascular complications during breast cancer (BC) treatment. The aim of this study was to investigate whether women diagnosed with BC exhibit a higher incidence of cardiovascular disease (CVD).
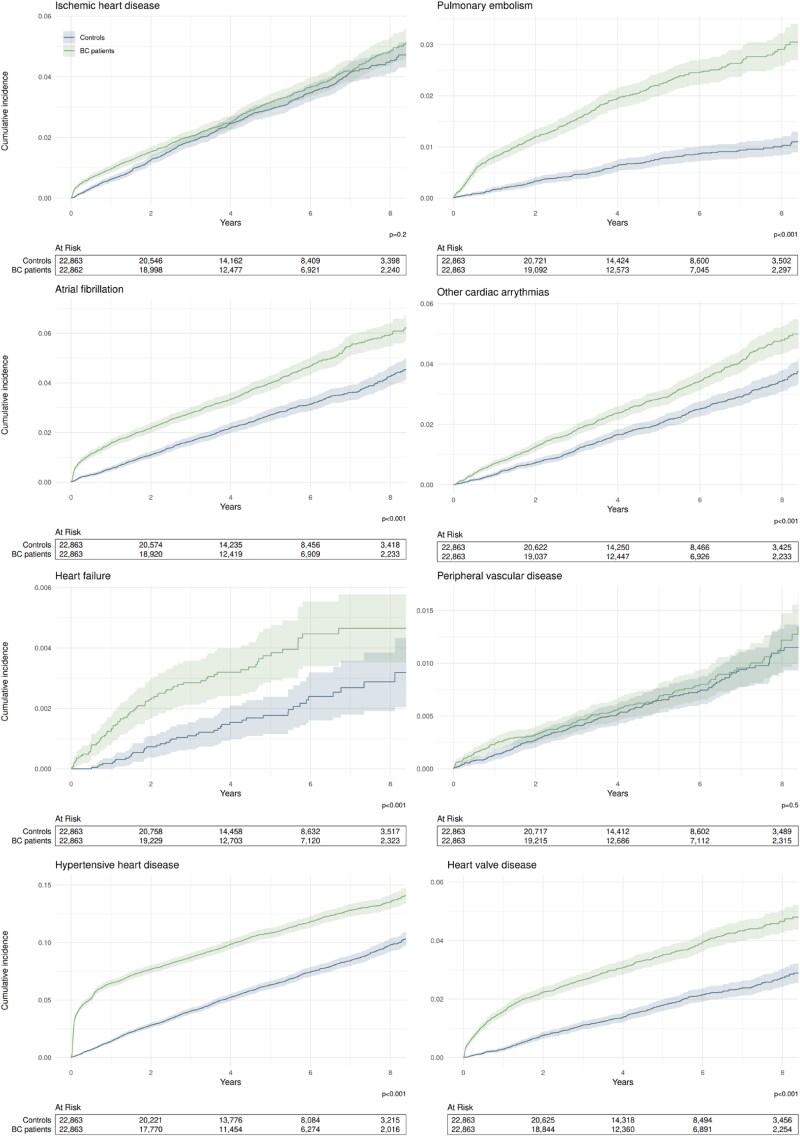
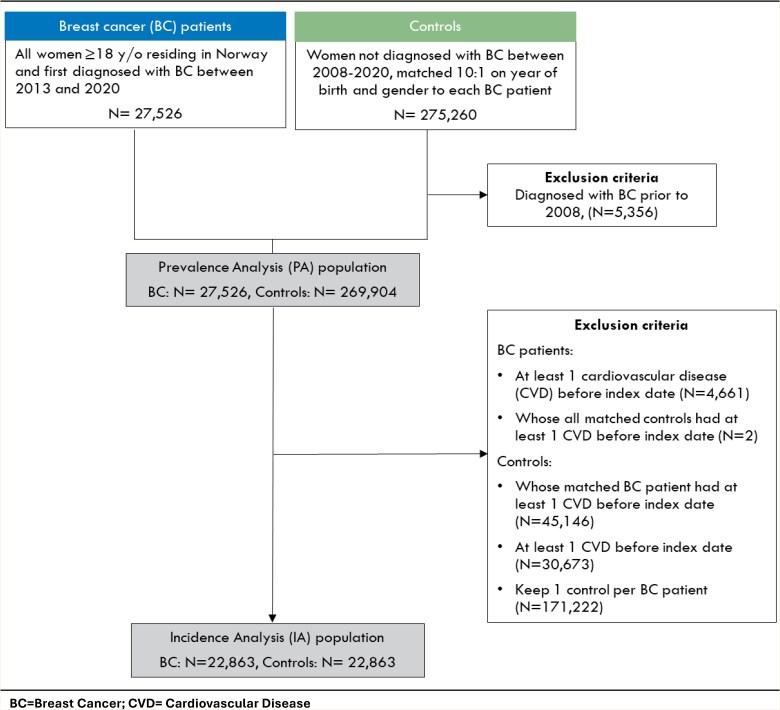
Methods and results: Matched cohort study. Using data from the Cancer Registry of Norway and the Norwegian Patient Registry, we created a nationwide cohort of women diagnosed with BC between 2013 and 2020 and age-matched controls (matching ratio 1:10). For BC patients, the index date was the date of their BC diagnosis. For controls, the index date was a random date within the index year of the matched BC patient. For eight selected CVDs, we compared the prevalence before BC diagnosis between cases and controls, as well as the overall incidence, hazard ratios (HRs), and cumulative incidences post BC diagnosis. Follow-up was through 2021. Our study population consisted of 27 526 BC patients and 269 904 matched controls. Among the subset of patients without CVD prior to index, BC patients had significantly increased overall and cumulative risk of pulmonary embolism (HR = 3.00, 95% CI: [2.51-3.59]), atrial fibrillation (1.53 [1.38-1.70]), other cardiac arrhythmias (1.43 [1.27-1.61]), heart failure (1.93 [1.33-2.80]), hypertensive heart disease (1.79 [1.67-1.91]), and heart valve disease (2.02 [1.79-2.27]).
Conclusion: In this contemporary cohort, BC patients still had an increased risk of several CVDs compared to age-matched controls. Further research is needed to determine the causes of this increased risk, but clinicians should be aware and optimize therapy accordingly.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


