Nicholas Frazzette, Jeffrey Ordner, Navneet Narula, Andre L Moreira, Christopher Y Park, Nicholas D Ward
{"title":"Co-occurrence of thymoma and acute T-lymphoblastic leukemia/lymphoma: a case report and literature review.","authors":"Nicholas Frazzette, Jeffrey Ordner, Navneet Narula, Andre L Moreira, Christopher Y Park, Nicholas D Ward","doi":"10.21037/med-24-23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A thymoma is a tumor originating from thymic epithelial cells variably associated with non-neoplastic lymphocytes. T-lymphoblastic leukemia/lymphoma (T-LBL) is thought to arise from precursor T-cells from bone marrow-derived hematopoietic stem cells that migrate to the thymus. While the association of secondary hematopoietic malignancies in thymoma is well established, only rarely in the literature have T-LBL and thymoma been seen in association and the relationship is poorly understood. Occasionally, distinction between the two can be difficult as immature lymphocytes in thymoma resemble T-LBL both morphologically and immunophenotypically. An accurate diagnosis is essential as treatments vary between these two entities.</p><p><strong>Case description: </strong>We present the interesting case of a 64-year-old male, former smoker, originally from Uzbekistan, with a mediastinal mass diagnosed as small cell carcinoma in his home country and treated with chemotherapy. After immigrating to the United States, a positron emission tomography (PET) scan demonstrated a large, metabolically active mediastinal mass. He presented to our institution where a biopsy with histomorphologic and immunohistochemical analysis was diagnostic of type B1 thymoma. He was lost to follow-up, but represented months later with B symptoms. Flow cytometry, cytogenetics, and bone marrow biopsy were diagnostic of T-LBL. Although he was started on chemotherapy, his disease progressed and he expired 6 months after initial presentation. Post-mortem analysis of the mediastinal mass revealed the co-occurrence of benign thymocytes and neoplastic T-LBL lymphoblasts, further confirmed as two distinct entities by T-cell receptor (TCR) sequencing.</p><p><strong>Conclusions: </strong>Co-occurrence of thymoma and T-LBL is a well-documented, though poorly understood, phenomenon. Literature review for this phenomenon reveals that type B thymoma is most commonly associated with T-LBL in these co-occurrences. Most cases are diagnosed synchronously, though in metachronous cases, the diagnosis of thymoma has always preceded the diagnosis of T-LBL. Of note, recently developed LMO2 immunohistochemical stain is positive in malignant lymphoblasts but negative in benign thymocytes, allowing for post-mortem evaluation of this case to be determined as a synchronous presentation. These entities are difficult to distinguish and require a multimodal diagnostic approach including histology, immunohistochemistry, flow cytometry, cytogenetics, and TCR sequencing.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"9 ","pages":"10"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11982990/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-24-23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A thymoma is a tumor originating from thymic epithelial cells variably associated with non-neoplastic lymphocytes. T-lymphoblastic leukemia/lymphoma (T-LBL) is thought to arise from precursor T-cells from bone marrow-derived hematopoietic stem cells that migrate to the thymus. While the association of secondary hematopoietic malignancies in thymoma is well established, only rarely in the literature have T-LBL and thymoma been seen in association and the relationship is poorly understood. Occasionally, distinction between the two can be difficult as immature lymphocytes in thymoma resemble T-LBL both morphologically and immunophenotypically. An accurate diagnosis is essential as treatments vary between these two entities.
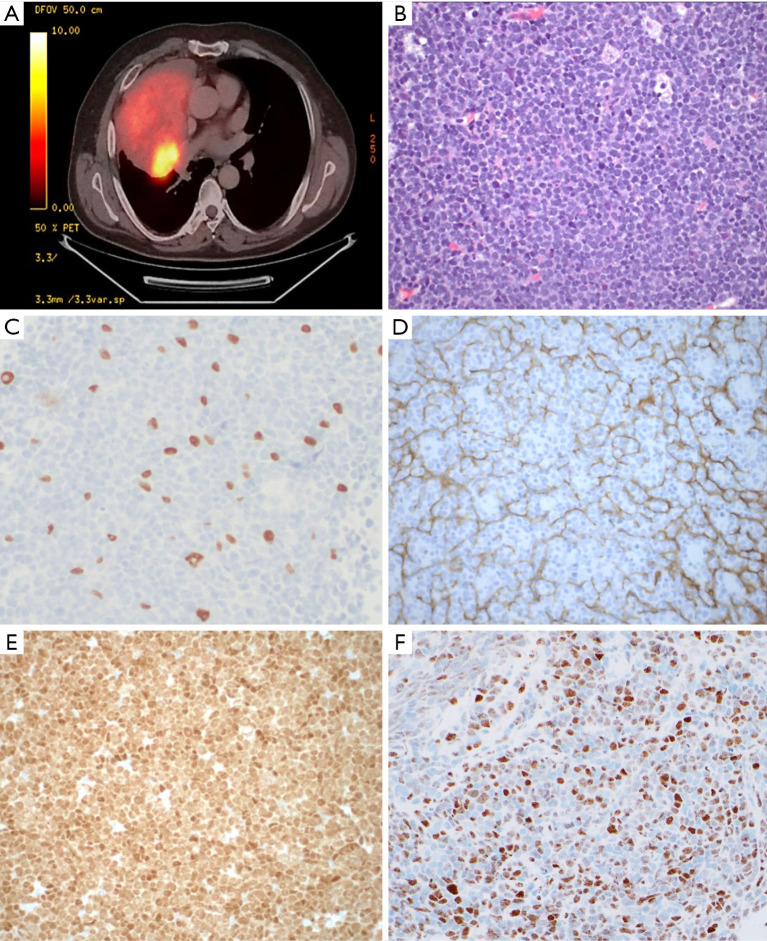
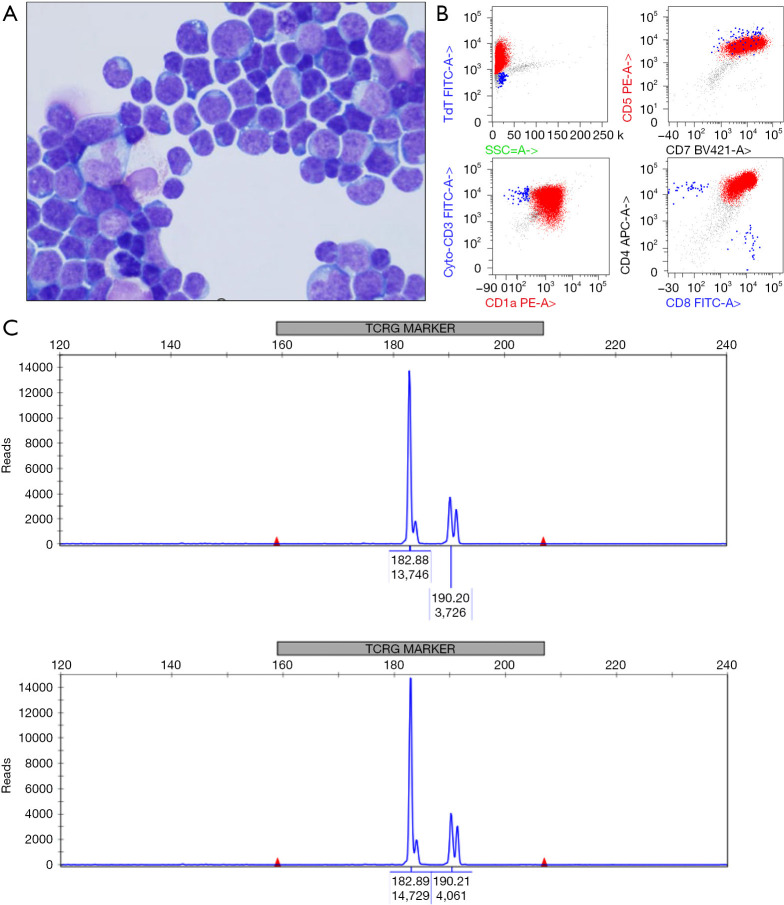
Case description: We present the interesting case of a 64-year-old male, former smoker, originally from Uzbekistan, with a mediastinal mass diagnosed as small cell carcinoma in his home country and treated with chemotherapy. After immigrating to the United States, a positron emission tomography (PET) scan demonstrated a large, metabolically active mediastinal mass. He presented to our institution where a biopsy with histomorphologic and immunohistochemical analysis was diagnostic of type B1 thymoma. He was lost to follow-up, but represented months later with B symptoms. Flow cytometry, cytogenetics, and bone marrow biopsy were diagnostic of T-LBL. Although he was started on chemotherapy, his disease progressed and he expired 6 months after initial presentation. Post-mortem analysis of the mediastinal mass revealed the co-occurrence of benign thymocytes and neoplastic T-LBL lymphoblasts, further confirmed as two distinct entities by T-cell receptor (TCR) sequencing.
Conclusions: Co-occurrence of thymoma and T-LBL is a well-documented, though poorly understood, phenomenon. Literature review for this phenomenon reveals that type B thymoma is most commonly associated with T-LBL in these co-occurrences. Most cases are diagnosed synchronously, though in metachronous cases, the diagnosis of thymoma has always preceded the diagnosis of T-LBL. Of note, recently developed LMO2 immunohistochemical stain is positive in malignant lymphoblasts but negative in benign thymocytes, allowing for post-mortem evaluation of this case to be determined as a synchronous presentation. These entities are difficult to distinguish and require a multimodal diagnostic approach including histology, immunohistochemistry, flow cytometry, cytogenetics, and TCR sequencing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


