Maria Fleseriu, Richard J Auchus, Wenyu Huang, Joanna L Spencer-Segal, Kevin C J Yuen, Kelley C Dacus, Julianne Padgett, Elizabeth K Babler, Ashis K Das, Cynthia Campos, Michael S Broder, Adriana G Ioachimescu
{"title":"Osilodrostat Treatment of Cushing Syndrome in Real-World Clinical Practice: Findings From the ILLUSTRATE study.","authors":"Maria Fleseriu, Richard J Auchus, Wenyu Huang, Joanna L Spencer-Segal, Kevin C J Yuen, Kelley C Dacus, Julianne Padgett, Elizabeth K Babler, Ashis K Das, Cynthia Campos, Michael S Broder, Adriana G Ioachimescu","doi":"10.1210/jendso/bvaf046","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>In clinical trials, osilodrostat (11β-hydroxylase inhibitor) effectively reduced cortisol levels in patients with endogenous Cushing syndrome (CS).</p><p><strong>Objectives: </strong>A real-world study (ILLUSTRATE) was conducted evaluating osilodrostat use in patients with various etiologies of CS in the United States.</p><p><strong>Methods: </strong>A retrospective chart-review study was conducted of adults with CS treated with osilodrostat between May 1, 2020, and October 29, 2021.</p><p><strong>Results: </strong>A total of 42 patients (Cushing disease, n = 34; CS due to adrenal adenoma, n = 5; ectopic adrenocorticotropin syndrome [EAS], n = 3) were included. Starting doses were 2 mg twice daily in 27/42 patients (64.3%), maintenance doses were 2 mg twice daily in 6 of 9 patients (66.7%) attaining them. During osilodrostat treatment, urinary free cortisol (UFC) decreased below the upper limit of normal (ULN) in 14 of 20 patients (70.0%) with pretreatment UFC greater than the ULN. Osilodrostat response was observed across a range of doses (2-20 mg/day). In Cushing disease, median UFC and late-night salivary cortisol decreased from 3.03 and 2.39 × ULN, respectively, to 0.71 and 1.13 × ULN at last assessment in those with available data (n = 17 and 8, respectively). UFC decreased in all patients with adrenal CS or EAS with available data (n = 2 each). There were no unexpected safety signals; the most common adverse events (incidence ≥20%) were fatigue, nausea, and lower-extremity edema. Glucocorticoid withdrawal syndrome and/or adrenal insufficiency were reported in 12 of 42 patients (28.6%) after osilodrostat initiation, resulting in treatment discontinuation in 4.</p><p><strong>Conclusion: </strong>In routine practice with dosing individualized according to clinical condition, response, and tolerability, osilodrostat was effective and well tolerated regardless of CS etiology and severity.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"9 5","pages":"bvaf046"},"PeriodicalIF":3.1000,"publicationDate":"2025-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11986586/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvaf046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Context: In clinical trials, osilodrostat (11β-hydroxylase inhibitor) effectively reduced cortisol levels in patients with endogenous Cushing syndrome (CS).
Objectives: A real-world study (ILLUSTRATE) was conducted evaluating osilodrostat use in patients with various etiologies of CS in the United States.
Methods: A retrospective chart-review study was conducted of adults with CS treated with osilodrostat between May 1, 2020, and October 29, 2021.
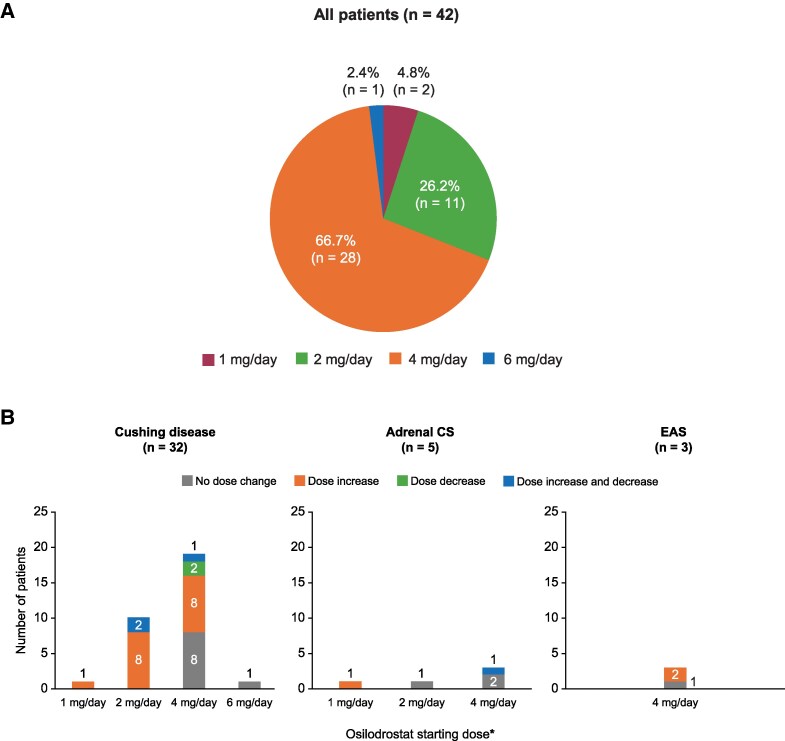
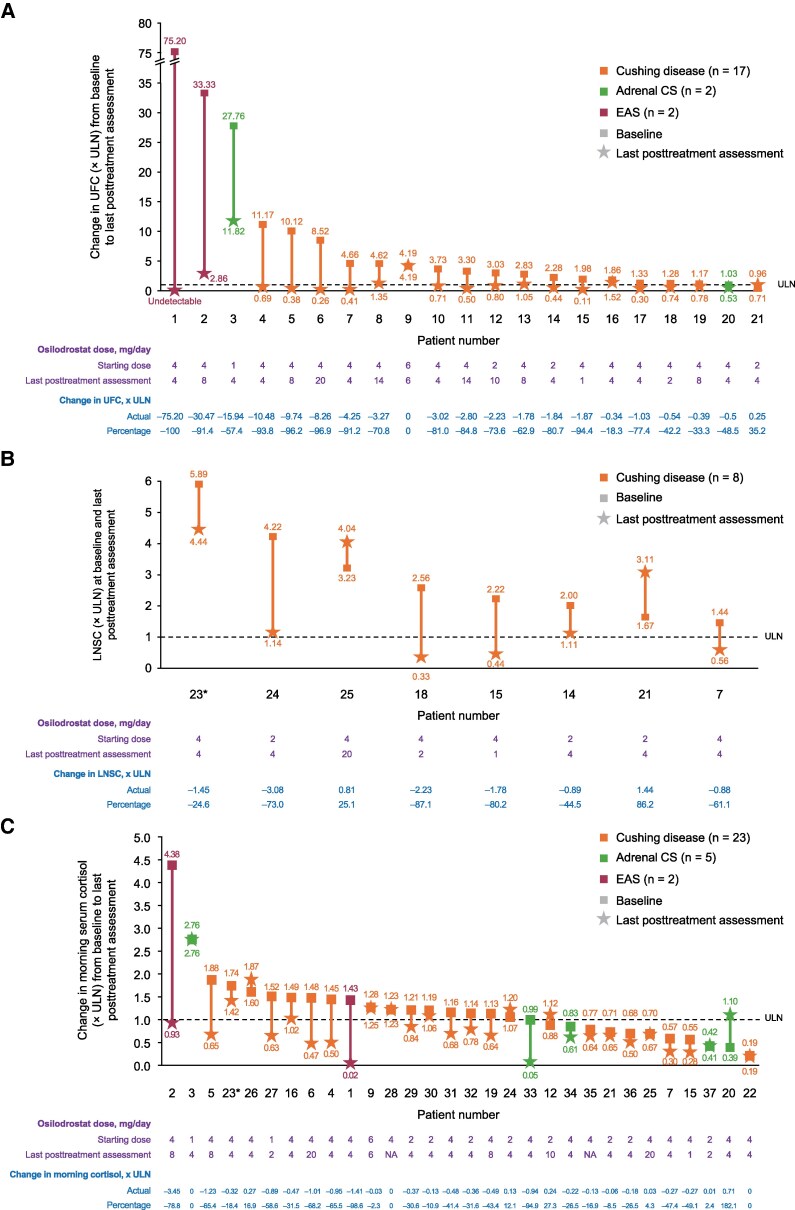
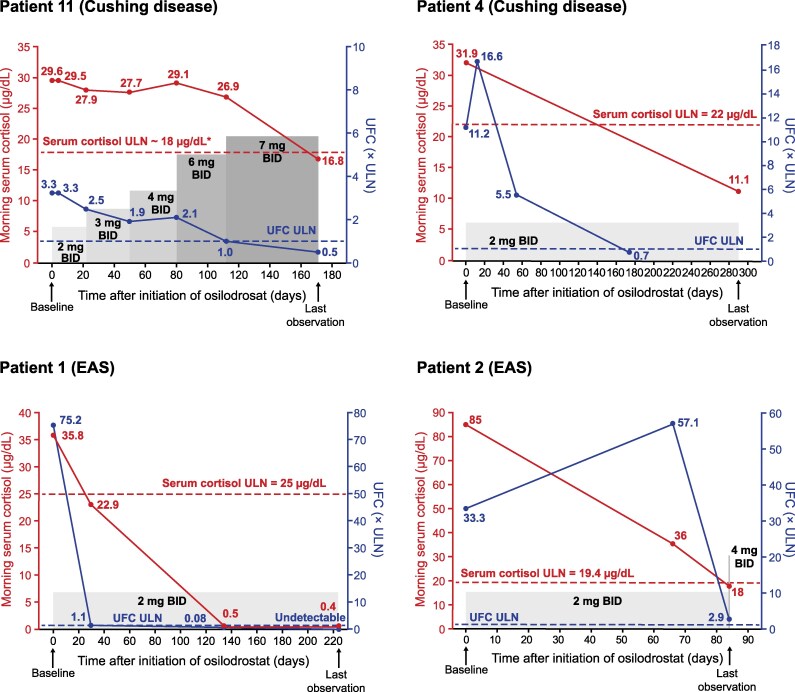
Results: A total of 42 patients (Cushing disease, n = 34; CS due to adrenal adenoma, n = 5; ectopic adrenocorticotropin syndrome [EAS], n = 3) were included. Starting doses were 2 mg twice daily in 27/42 patients (64.3%), maintenance doses were 2 mg twice daily in 6 of 9 patients (66.7%) attaining them. During osilodrostat treatment, urinary free cortisol (UFC) decreased below the upper limit of normal (ULN) in 14 of 20 patients (70.0%) with pretreatment UFC greater than the ULN. Osilodrostat response was observed across a range of doses (2-20 mg/day). In Cushing disease, median UFC and late-night salivary cortisol decreased from 3.03 and 2.39 × ULN, respectively, to 0.71 and 1.13 × ULN at last assessment in those with available data (n = 17 and 8, respectively). UFC decreased in all patients with adrenal CS or EAS with available data (n = 2 each). There were no unexpected safety signals; the most common adverse events (incidence ≥20%) were fatigue, nausea, and lower-extremity edema. Glucocorticoid withdrawal syndrome and/or adrenal insufficiency were reported in 12 of 42 patients (28.6%) after osilodrostat initiation, resulting in treatment discontinuation in 4.
Conclusion: In routine practice with dosing individualized according to clinical condition, response, and tolerability, osilodrostat was effective and well tolerated regardless of CS etiology and severity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


